Tonsillitis Management: Practical Step-Up Approach from OPD to Emergency
On this page
Tonsillitis Management Sheet
| Situation | Setting | Key findings | Treatment | Follow-up / next step |
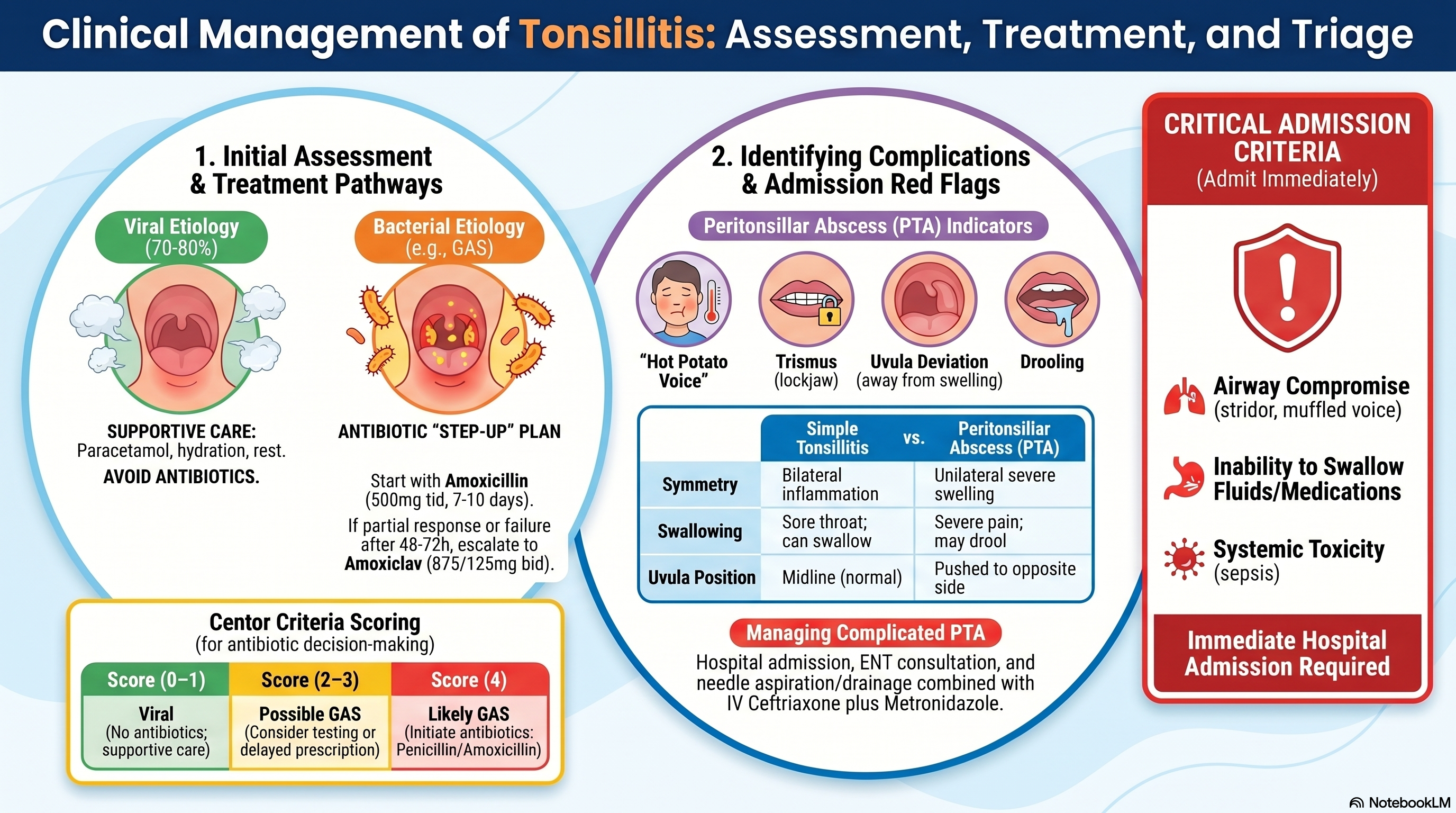
| Likely viral tonsillitis | OPD | mild sore throat, cough/rhinorrhea present, able to swallow, no red flags | No antibiotic. Supportive care: Paracetamol (500 mg), 1–2 tab po q6h prn, warm saline gargle, hydration, rest | Return if worse, high fever, cannot swallow, unilateral swelling |
| Likely bacterial tonsillitis (GAS pattern) | OPD | fever, tonsillar exudate, tender anterior cervical nodes, no cough, able to swallow, no airway issue | Amoxicillin (500 mg), 1×3 po, for 7 days in your local practical approach | Reassess if not improving after 48–72 hr or if worse |
| Not improving but still no abscess signs, still able to swallow | OPD | persistent fever/sore throat, no trismus, no uvula deviation, no drooling, no hot potato voice | Shift to Amoxiclav (875/125 mg), 1×2 po, for 7–14 days | Review in 48–72 hr |
| Suspected peritonsillar cellulitis / early complication | Usually IPD or urgent ENT evaluation | worsening unilateral pain, asymmetry, severe odynophagia, but abscess not yet certain | ENT assessment, consider IV treatment depending on severity | Watch closely for abscess signs |
| Peritonsillar abscess (PTA) | IPD / ED / ENT consult | trismus, hot potato voice, uvula deviation, unilateral tonsillar bulge, drooling, severe pain | Needle aspiration / I&D + Ceftriaxone (2 g), 1×1 IV plus Metronidazole (500 mg), 1×3 IV | Step down to Amoxiclav (875/125 mg), 1×2 po, 10–14 days when improved |
Practical step-up plan
| Step | Drug | Ready-to-use prescription |
| First-line in your practice | Amoxicillin | Amoxicillin (500 mg), 1×3 po, for 7–14 days |
| If partial response / failure and still uncomplicated | Amoxiclav | Amoxiclav (875/125 mg), 1×2 po, for 7–14 days |
| If abscess / severe complicated infection | IV regimen | Ceftriaxone (2 g), 1×1 IV + Metronidazole (500 mg), 1×3 IV |
When to continue up to 14 days
Use longer total duration up to 10–14 days when:
- symptoms improve slowly
- infection is more severe
- there is recurrent disease
- step-up to amoxiclav
- after drainage of PTA
Admit the patient if any of these are present
| Admission concern | What to look for |
| Airway compromise | drooling, stridor, muffled voice, respiratory distress, kissing tonsils |
| Cannot swallow / dehydration | unable to take PO meds or fluids, dry mucosa, low urine output, lethargy |
| Severe systemic toxicity / sepsis | high fever, tachycardia, hypotension, rigors, confusion, toxic appearance |
| Suspected peritonsillar abscess | unilateral swelling, uvula deviation, trismus, hot potato voice, drooling |
| Deep neck infection concern | neck swelling, neck stiffness, severe pain, toxic appearance |
| Failure of outpatient treatment | worsening or no improvement after 48–72 hr of appropriate antibiotics |
| Immunocompromised host | uncontrolled DM, chemotherapy, advanced HIV, chronic steroid use |
| Need procedure / uncertain diagnosis | possible abscess needing aspiration, need CT neck, ENT procedure |
How to tell it has turned into an abscess
| Simple tonsillitis | Peritonsillar abscess |
| usually bilateral inflammation | usually unilateral severe swelling |
| sore throat but can usually swallow | marked odynophagia, may drool |
| no trismus | trismus present |
| no uvula deviation | uvula pushed away |
| normal voice or mild pain voice | hot potato voice |
| responds to oral meds | often worsening despite antibiotics |
Quick note for exams
- Simple bacterial tonsillitis: oral antibiotic is enough
- Not improving: reassess, do not escalate blindly
- PTA: drainage + IV antibiotics
- Ceftriaxone alone is not enough for PTA → add metronidazole
One-line quick orders
- Uncomplicated bacterial tonsillitis: Amoxicillin (500 mg), 1×3 po, for 7 days
- If failed, still uncomplicated: Amoxiclav (875/125 mg), 1×2 po, for 7–14 days
- If PTA suspected: Admit, ENT consult, drainage, Ceftriaxone (2 g), 1×1 IV + Metronidazole (500 mg), 1×3 IV
1. Definition
Tonsillitis = inflammation of the palatine tonsils
- Most common cause → viral (70–80%)
- Bacterial → mainly Group A Streptococcus (GAS)
2. Clinical Classification
🔹 Acute Tonsillitis
- Duration < 14 days
- Viral vs bacterial
🔹 Recurrent Tonsillitis
- ≥ 7 episodes/year OR
- ≥ 5/year for 2 years OR
- ≥ 3/year for 3 years
🔹 Complicated Tonsillitis
- Peritonsillar abscess (PTA)
- Deep neck infection
3. Clinical Assessment
Symptoms
- Sore throat
- Fever
- Odynophagia
- Dysphagia
Signs
- Tonsillar erythema ± exudate
- Tender cervical lymph nodes
- Fever
🎯 Centor Criteria (IMPORTANT EXAM TOOL)
| Criteria | Score |
| Fever >38°C | +1 |
| Tonsillar exudate | +1 |
| Tender anterior cervical LN | +1 |
| No cough | +1 |
Interpretation:
- 0–1 → Viral → NO antibiotics
- 2–3 → Consider test or delayed Rx
- 4 → Likely GAS → Give antibiotics
4. Management Approach
🏥 Step 1: Decide OPD vs IPD
Think of this as 3 domains: 👉 Airway 👉 Ability to maintain intake 👉 Severity/systemic risk
✅ OPD (Outpatient Management)
You can safely treat as OPD ONLY if ALL are stable
1. Airway is safe
- No stridor
- No drooling
- No voice change (no “hot potato voice”)
- No significant tonsillar enlargement causing obstruction
👉 Meaning: airway is not threatened
2. Patient can maintain oral intake
- Able to swallow fluids and medications
- Mild–moderate odynophagia only
- No signs of dehydration
👉 Clinically:
- moist mucous membranes
- normal urine output
- not lethargic
3. Mild–moderate disease severity
- Fever but not a toxic appearance
- Stable vital signs:
- HR < 100–110
- BP stable
- RR normal
- Pain controlled with oral meds
4. No complication suspected
- Bilateral tonsillar inflammation (typical)
- No asymmetry
- No uvula deviation
- No trismus
5. No high-risk host
- Immunocompetent
- No uncontrolled diabetes
- No chemotherapy / HIV advanced
6. Good follow-up reliability
- Can return if worse
- Has access to care within 24–48 hrs
🚨 IPD (Admission Criteria – VERY IMPORTANT)
👉 You only need ONE major criterion to be admitted 🔴 1. AIRWAY COMPROMISE (MOST IMPORTANT)
Signs:
- Drooling → cannot swallow saliva
- Stridor → upper airway obstruction
- Muffled voice (“hot potato voice”)
- Severe tonsillar enlargement (“kissing tonsils”)
- Respiratory distress
👉 PathophysiologySwelling/abscess → narrowing of oropharynx → risk of sudden airway obstruction
👉 Exam pearlIf airway risk → DO NOT delay → admit immediately
🔴 2. DEHYDRATION / CANNOT SWALLOW
Clinical signs:
- Cannot take oral meds/fluids
- Dry mucosa
- Reduced urine output
- Tachycardia
👉 Reason:
- Odynophagia → ↓ intake → dehydration
- Oral antibiotics ineffective → need IV route
🔴 3. SEVERE SYSTEMIC TOXICITY / SEPSIS
Signs:
- High fever (>39°C)
- Tachycardia (>110–120)
- Hypotension
- Confusion / lethargy
- Rigors
👉 Think:
- Bacteremia
- Deep infection
🔴 4. SUSPECTED COMPLICATION (VERY HIGH-YIELD)
Peritonsillar Abscess (PTA)
- Unilateral swelling
- Trismus
- Uvula deviation
- Severe pain
Deep Neck Infection
- Neck swelling
- Neck stiffness
- Toxic appearance
👉 These require:
- Imaging
- Drainage
- IV antibiotics
🔴 5. FAILURE OF OUTPATIENT TREATMENT
- No improvement after 48–72 hours of appropriate antibiotics
- Worsening symptoms
👉 Reason:
- Wrong diagnosis
- Resistant bacteria
- Abscess formation
🔴 6. IMMUNOCOMPROMISED PATIENT
Examples:
- Diabetes mellitus (poor control)
- HIV/AIDS
- Chemotherapy
- Long-term steroids
👉 Why admit?
- Higher risk of:
- Rapid progression
- Atypical infection
- Sepsis
🔴 7. DIAGNOSTIC UNCERTAINTY / NEED PROCEDURE
- Cannot differentiate cellulitis vs abscess
- Need:
- Needle aspiration
- CT neck
💊 Step 2: Treatment
A. Viral Tonsillitis (MOST COMMON)
❌ NO antibiotics
✅ Supportive Treatment
- Paracetamol (500 mg), 1–2 tab q6h prn po
- Ibuprofen (400 mg), tid po
- Warm saline gargle
- Hydration, rest
👉 Guideline: NICE / CDC → avoid unnecessary antibiotics
B. Bacterial Tonsillitis (GAS)
✅ First-line (Definitive Treatment)
- Penicillin V (500 mg), 1×2 po, for 10 days
OR
- Amoxicillin (500 mg), 1×3 po, for 10 days
💡 Why?
- Narrow spectrum
- Effective vs GAS
- Prevent rheumatic fever
👉 Guideline: CDC, IDSA
❌ What NOT to use
- Broad-spectrum (amoxiclav, ceftriaxone) ❌ unnecessary
- Short duration ❌ increases recurrence
But in practice, we use Amoxiclav (875/125 mg), 1×2 po, 7–14 days, if Amoxicillin (500 mg), 1×3 po, for 7 days, the result is Fail.
If Penicillin Allergy
- Clindamycin (300 mg), 1×4 po, for 10 days
OR
- Azithromycin (500 mg), 1×1 po, for 5 days
C. Not Improving After 48–72 hrs
👉 Reassess:
- Compliance?
- Viral infection?
- Infectious mononucleosis?
- Complication (PTA)?
Management:
- ❌ Do NOT escalate blindly
- ✅ Re-evaluate diagnosis
🚨 D. Complicated: Peritonsillar Abscess (PTA) Key Signs
- Trismus
- Hot potato voice
- Uvula deviation
- Unilateral swelling
- Drooling
Management
Setting: IPD + ENT consult
✅ Definitive Treatment
- Needle aspiration / incision & drainage
✅ Antibiotics
- Ceftriaxone (2 g), 1×1 IVPLUS
- Metronidazole (500 mg), 3×1 IV
Step-down:
- Amoxiclav (875/125 mg), 1×2 po, 10–14 days
❌ Exam mistake
- Antibiotics alone ❌
- No drainage ❌
5. Investigations
Routine (NOT always needed)
- Clinical diagnosis
If needed:
- Throat swab (GAS)
- CBC (infection)
- Monospot (EBV)
If an abscess is suspected:
- Needle aspiration
- CT neck with contrast
6. Complications
- Peritonsillar abscess
- Rheumatic fever
- Post-streptococcal glomerulonephritis
- Deep neck infection
7. Indication for Tonsillectomy
Paradise Criteria
- ≥7 episodes/year
- ≥5/year for 2 years
- ≥3/year for 3 years
8. Follow-up
- Review in 2–3 days if worsening
- Return immediately if:
- breathing difficulty
- cannot swallow
- severe pain
HIGH-YIELD SUMMARY
👉 Most tonsillitis = viral → supportive only 👉 GAS = Penicillin V 10 days 👉 Not improving = reassess, not escalate blindly 👉 PTA = Drain + IV antibiotics (ceftriaxone + metronidazole) 👉 Admit if airway / dehydration / complication