Osgood-Schlatter Disease: Diagnosis, Pathophysiology, and Management
On this page
Osgood-Schlatter disease (OSD) is one of the most common causes of anterior knee pain in adolescents, particularly those who are physically active. It is a benign, self-limiting condition associated with growth spurts and repetitive stress on the knee joint. Understanding its pathophysiology, diagnosis, investigation, and management is essential for both clinical practice and medical examinations.
Introduction
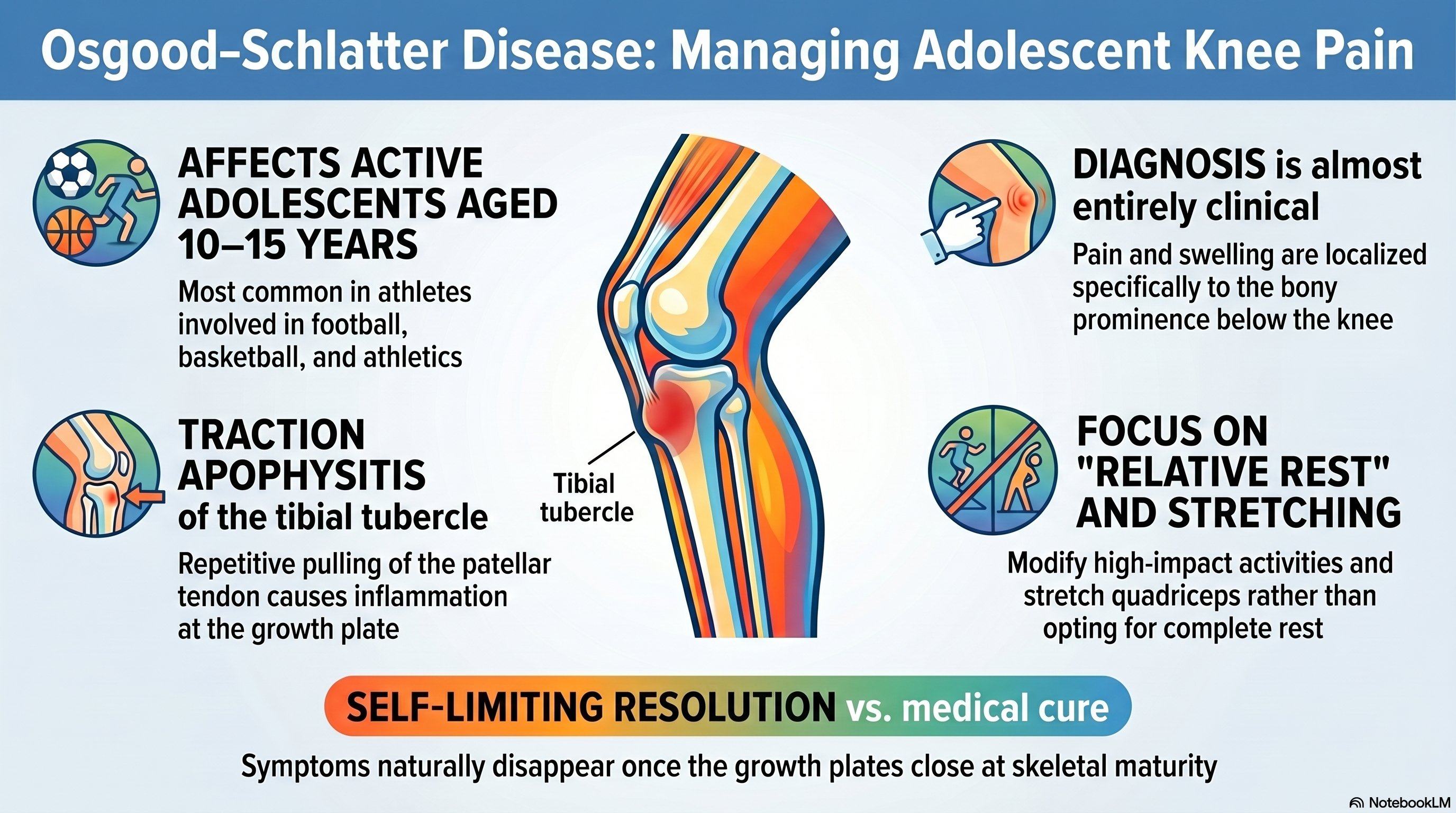
Osgood-Schlatter disease typically affects adolescents aged 10–15 years, especially those involved in sports such as football, basketball, volleyball, and athletics. It presents with pain and swelling over the tibial tubercle, the bony prominence just below the knee.
This condition is not a true “disease” in the infectious sense but rather an overuse injury involving the growth plate (apophysis) of the tibial tubercle.
Pathophysiology
The key mechanism in Osgood-Schlatter disease is repetitive traction (pulling force) at the insertion of the patellar tendon on the tibial tubercle.
Step-by-step mechanism:
- During adolescence, the tibial tubercle is still developing (apophysis).
- The quadriceps muscle contracts during activities like running and jumping.
- This contraction pulls on the patellar tendon.
- The patellar tendon transmits force to the tibial tubercle.
- Repeated stress leads to:
- Microtrauma
- Inflammation
- Possible fragmentation of the apophysis
Key Concept:
👉 Traction apophysitis = inflammation due to repetitive pulling at a growth plate
Why adolescents?
- Growth plates are weaker than tendons
- Rapid bone growth → tight quadriceps → increased tension
Clinical Diagnosis
Osgood-Schlatter disease is primarily a clinical diagnosis.
Typical Patient Profile:
- Age: 10–15 years
- Active in sports
- Gradual onset of knee pain
Symptoms:
- Anterior knee pain
- Pain localized to the tibial tubercle
- Worsens with:
- Running
- Jumping
- Kneeling
- Squatting
- Improves with rest
Physical Examination:
- Tenderness over tibial tubercle
- Prominent or swollen tibial tubercle
- Pain with resisted knee extension
- Tight quadriceps/hamstrings
Red Flags (NOT typical for OSD):
- Fever
- Night pain
- Severe acute trauma
- Systemic symptoms
👉 If present → consider other diagnoses
Differential Diagnosis (Important for Exams)
- Patellar tendinopathy (Jumper’s knee)
- Sinding-Larsen-Johansson syndrome
- Tibial tubercle avulsion fracture
- Osteomyelitis
- Bone tumors (rare but important to rule out)
Investigations
1. Clinical Diagnosis (Most Important)
- No investigation needed in classic cases
2. Imaging
X-ray (if needed)
Indications:
- Atypical presentation
- Severe pain
- Trauma history
- Rule out fracture
Findings:
- Fragmentation of the tibial tubercle
- Soft tissue swelling
3. Laboratory Tests
❌ Not routinely required
Only if:
- Suspected infection (e.g., osteomyelitis)
- Systemic symptoms
Management
Osgood-Schlatter disease is self-limiting, so treatment focuses on symptom control and activity modification.
1. Management Setting
✅ Outpatient Department (OPD) (No need for hospital admission)
2. Definitive Treatment
There is no “curative drug” because the condition resolves with skeletal maturity.
Activity Modification
- Reduce high-impact activities (running, jumping)
- Avoid pain-triggering movements
👉 NOT complete rest, but “relative rest.”
3. Supportive Treatment
Pain Management
- Paracetamol (500 mg) 1×3 po pc for 5–7 days OR
- Ibuprofen (400 mg) 1×3 po pc for 5–7 days
(Guideline: Standard pediatric orthopedic and pain management principles )
Ice Therapy
- Apply ice 15–20 minutes after activity
- Reduces inflammation
Physiotherapy
- Quadriceps stretching
- Hamstring stretching
- Strengthening exercises
👉 Reduces tension on the tibial tubercle
Support Devices
- Patellar tendon strap
- Knee brace (optional)
4. What NOT to Do (Exam Pearls)
❌ No antibiotics → not an infection ❌ No steroids → not inflammatory systemic disease ❌ No surgery (in most cases)
👉 But in your exam, if forced to choose medication → NSAIDs like ibuprofen are correct
5. Surgical Management (Rare)
Indications:
- Persistent symptoms after skeletal maturity
- Severe ossicle formation
Prognosis
- Excellent prognosis
- Symptoms resolve with growth plate closure
- May leave:
- Prominent tibial tubercle (cosmetic)
Follow-Up Plan
- Follow-up every 4–6 weeks
- Assess:
- Pain level
- Activity tolerance
- Gradual return to sports when pain-free
Patient Education
- Condition is benign and self-limiting
- Avoid pushing through pain
- Continue stretching exercises
- Return if:
- Pain worsens
- Swelling increases
- New symptoms appear
Key Exam Pearls
- 📌 Age 10–15 + sports + tibial tubercle pain → think OSD
- 📌 Diagnosis = clinical
- 📌 Treatment = activity modification + NSAIDs
- 📌 Self-limiting → resolves after growth
Conclusion
Osgood-Schlatter disease is a classic example of a growth-related overuse injury in adolescents. Recognizing its characteristic presentation allows clinicians to avoid unnecessary investigations and provide effective reassurance and conservative management. For medical students, it is a high-yield topic frequently tested in exams due to its clear clinical features and straightforward management.