Alcohol Intoxication (เมาเหล้า เมาสุรา) Management: ER Approach, Red Flags, and Safe Discharge Criteria
On this page
📄 ER Order Sheet: Suspected Alcohol Intoxication
🧾 Initial Orders
- DTX (capillary blood glucose) – stat
- Vital signs monitoring
- Observe in ER (serial mental status + airway monitoring)
💉 Medications
- Thiamine 100 mg IV stat OR
- Vitamin B complex (containing thiamine 100 mg) IV stat
💧 IV Fluids (ONLY if indicated)
- 0.9% NSS 1000 mL IV
- Rate: 80–100 mL/hr OR adjust based on clinical status
- Indication: dehydration / vomiting / poor oral intake
🧪 Labs (ONLY if clinically indicated)
(Do NOT send all routinely — choose based on case)
- CBC
- BUN, Creatinine
- Electrolytes (Na, K, Cl, HCO₃)
- Calcium, Magnesium, Phosphate
🔍 Additional Workup (if red flags)
- CXR → if aspiration / pneumonia suspected
- CT brain → if trauma / focal deficit / unexplained AMS
- Lactate → if concern for sepsis or hypoperfusion
- UA → if urinary symptoms
👀 Monitoring
- Reassess mental status every 1–2 hours
- Monitor for:
- Airway compromise
- Hypoxia
- Worsening consciousness
- Signs of withdrawal (tremor, agitation, tachycardia)
✅ Disposition Criteria (Discharge when ALL met)
- Awake and oriented
- Stable vital signs
- Able to walk safely
- Tolerating oral intake
- No underlying pathology identified
🚫 Do NOT
- ❌ Do NOT give dextrose if DTX normal
- ❌ Do NOT send full labs in every simple intoxication
- ❌ Do NOT assume all AMS = alcohol
- ❌ Do NOT give fixed IV fluid in all patients
💡 One-line version (EXAM STYLE)
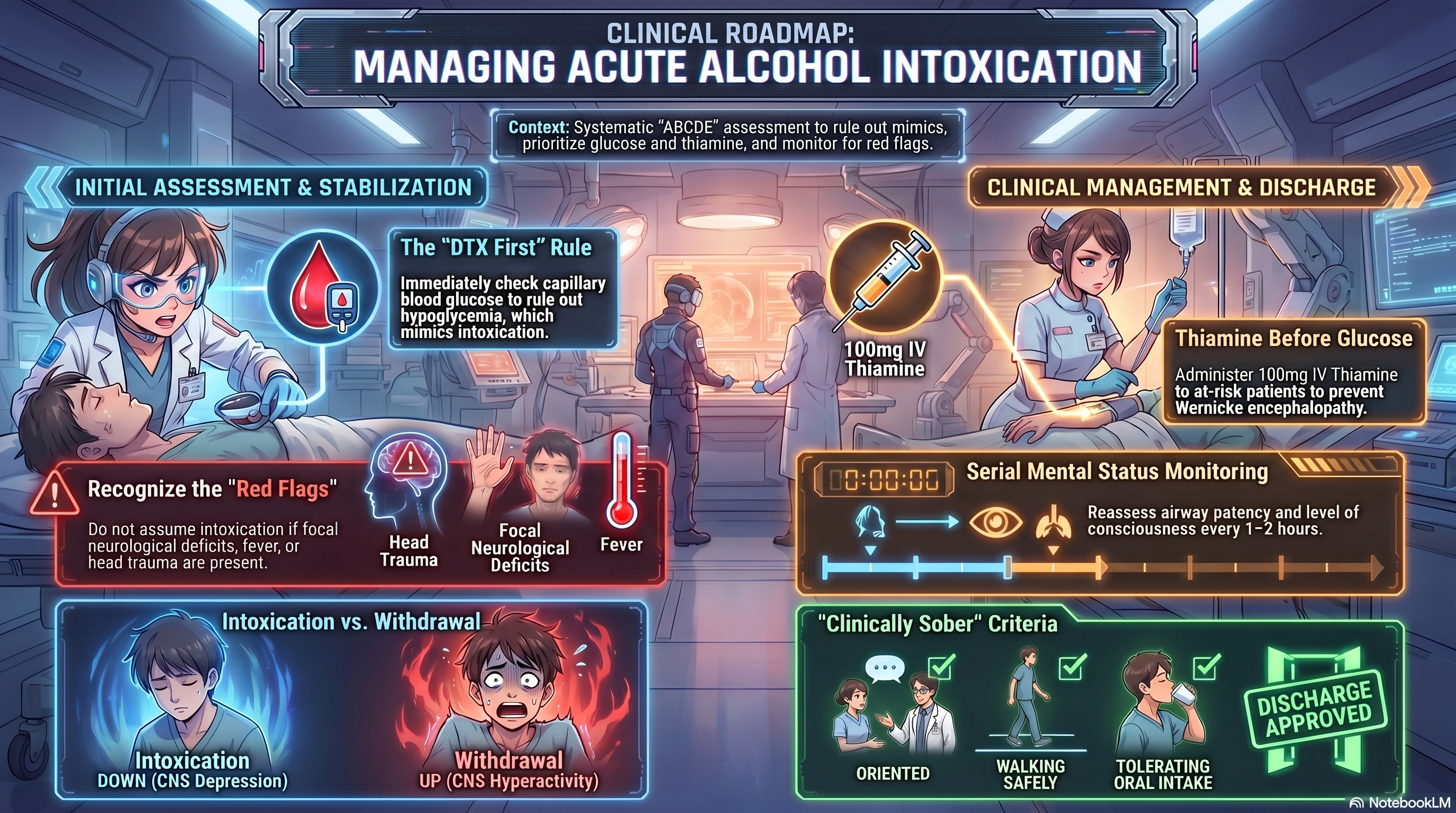
DTX → Observe → Thiamine 100 mg IV → IV fluids if dehydrated → Targeted labs if indicated → Reassess → Discharge when clinically sober
Approach to Patients Presenting with Alcohol Intoxication in the Emergency and Outpatient Setting
Alcohol intoxication is one of the most common presentations in both emergency departments (ER) and outpatient settings. While many cases are uncomplicated and self-limiting, clinicians must approach every patient carefully, as serious conditions can mimic or coexist with alcohol intoxication.
This article provides a practical, guideline-based approach for evaluating and managing patients who present with suspected alcohol intoxication.
Understanding Alcohol Intoxication
Acute alcohol intoxication results from the central nervous system (CNS) depressant effects of ethanol. Clinical features typically progress depending on the amount consumed and patient tolerance.
Common findings include:
- Slurred speech
- Impaired coordination and gait instability
- Altered judgment and behavior
- Drowsiness or decreased level of consciousness
In severe cases:
- Respiratory depression
- Coma
- Risk of aspiration
Alcohol intoxication is primarily a clinical diagnosis, but it should always be considered a diagnosis of exclusion in patients with altered mental status.
Initial Assessment
The first priority is a structured and systematic evaluation.
1. Primary Assessment (ABCDE)
- Airway: Ensure patency and protection
- Breathing: Assess respiratory rate and oxygen saturation
- Circulation: Check blood pressure and perfusion
- Disability: Evaluate level of consciousness (e.g., GCS)
- Exposure: Look for trauma, injuries, or signs of infection
2. Immediate Bedside Test
- Capillary blood glucose (DTX) must be checked in all patients→ Hypoglycemia can mimic alcohol intoxication and must be treated immediately.
When Is It Truly Alcohol Intoxication?
A diagnosis of uncomplicated alcohol intoxication becomes more likely when:
- There is a clear history of recent alcohol intake
- Clinical signs are consistent with CNS depression
- No focal neurological deficits are present
- Vital signs are stable
- Blood glucose is normal
- The patient improves over time with observation
Red Flags: When It Is NOT Just Alcohol
Clinicians must actively look for alternative or additional diagnoses.
Do NOT assume alcohol intoxication if any of the following are present:
- Persistent or worsening altered mental status
- Focal neurological deficits (e.g., weakness, facial droop)
- Signs of head trauma
- Hypoxia or abnormal respiratory pattern
- Fever or hypothermia
- Severe abdominal pain or persistent vomiting
- Seizures
- Failure to improve with time
Possible alternative diagnoses include:
- Hypoglycemia
- Traumatic brain injury
- Stroke
- Sepsis
- Meningitis or encephalitis
- Drug or toxin co-ingestion
- Hepatic encephalopathy
- Alcoholic ketoacidosis
Differentiating Alcohol Intoxication from Alcohol Withdrawal
This distinction is critical and commonly tested in clinical exams.
Alcohol Intoxication (CNS Depression)
- Drowsiness
- Slurred speech
- Poor coordination
- Decreased responsiveness
Alcohol Withdrawal (CNS Hyperactivity)
- Tremors
- Anxiety and agitation
- Sweating
- Tachycardia and hypertension
- Insomnia
- Hallucinations
- Seizures (in severe cases)
A key clinical clue:
- Intoxication = “down” (depressed)
- Withdrawal = “up” (overactive)
Supportive Management
Most patients with uncomplicated alcohol intoxication require supportive care only.
Observation
- Monitor vital signs regularly
- Reassess mental status frequently
- Ensure airway protection
Hydration
- Administer IV fluids if dehydrated or unable to tolerate oral intake
Nutrition
- Start oral fluids and food when the patient is alert and not vomiting
Role of Vitamin B Complex
Patients with chronic alcohol use are at risk of thiamine deficiency, which can lead to Wernicke encephalopathy, a potentially life-threatening neurological condition.
Indications for Vitamin B Complex
- Chronic or heavy alcohol use
- Malnutrition or poor oral intake
- Recurrent vomiting
- Altered mental status
- Suspected Wernicke encephalopathy
Recommended Use
- Vitamin B complex (containing thiamine 100 mg)
- Administer intravenously or intramuscularly, single dose initially
- Continue daily dosing if the patient is admitted or at ongoing risk
Important Clinical Pearl
- If intravenous glucose is required, thiamine should be given before or with glucose in at-risk patients to prevent worsening neurological injury.
When to Investigate Further
Laboratory and imaging studies are not required for every patient, but should be considered if:
- The clinical picture is unclear
- There are red flag symptoms
- The patient does not improve with observation
- There is suspicion of complications or alternative diagnoses
Possible investigations include:
- Electrolytes and renal function
- Liver function tests
- Blood gas analysis
- Urinalysis
- Chest imaging (if aspiration is suspected)
- Brain imaging (if trauma or neurological deficit is present)
Criteria for Safe Discharge
A patient can be discharged when they are clinically sober, meaning:
- Fully awake and oriented
- Able to communicate appropriately
- Able to sit, stand, and walk safely
- Vital signs are stable
- No underlying medical condition requiring treatment is identified
Additionally:
- The patient should have a safe environment for discharge
- Ideally, discharge with a responsible caregiver
Follow-Up and Prevention
Alcohol intoxication is often a marker of underlying alcohol misuse.
Consider:
- Brief counseling on alcohol use
- Referral to addiction services if appropriate
- Education on the risks of heavy drinking
Key Takeaways
- Alcohol intoxication is a diagnosis of exclusion
- Always check blood glucose first
- Distinguish between intoxication (depression) and withdrawal (hyperactivity)
- Use Vitamin B complex (thiamine 100 mg) in at-risk patients
- Observe and reassess — improvement over time supports intoxication
- Do not miss life-threatening conditions that mimic alcohol intoxication