Anaphylaxis: Emergency Diagnosis and Immediate Management (High-Yield Guide)
On this page
A) Clinical diagnosis
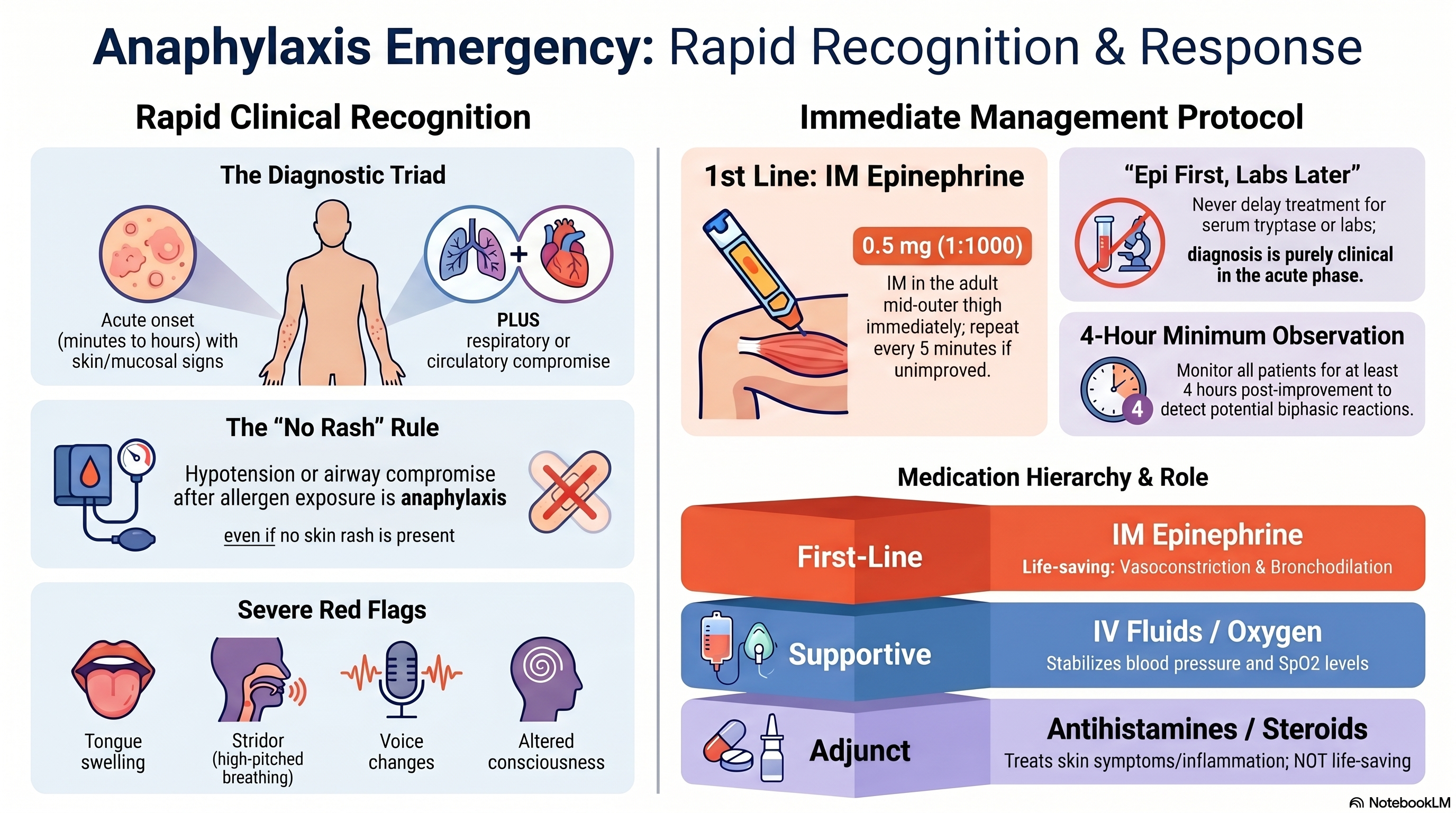
Think anaphylaxis if acute onset (minutes to hours) after a likely trigger with:
- Skin/mucosal signs: urticaria, flushing, lip/tongue swelling, angioedemaplus
- Respiratory compromise: wheeze, dyspnea, stridor, hoarsenessor
- Circulatory compromise: hypotension, syncope, shock
Also call it anaphylaxis if there is hypotension / bronchospasm / laryngeal edema after allergen exposure even without rash.
B) Physical examination
Focus on ABCDE
Airway
- lip/tongue swelling → angioedema
- uvular edema → angioedema
- hoarseness
- stridor
Breathing
- tachypnea
- wheeze
- hypoxia
- respiratory distress
Circulation
- tachycardia
- hypotension
- weak pulse
- poor perfusion
Disability
- dizziness
- confusion
- syncope
Exposure
- urticaria
- flushing
- angioedema
C) Labs / workup to send
Do not delay treatment for labs.
Support diagnosis
- Serum tryptase: immediate sample, repeat later if admitted
Assess severity
- CBC
- electrolytes
- BUN/Cr
- glucose
- ABG if severe
- ECG / cardiac monitor if unstable or IV adrenaline infusion needed
Later
- allergy workup / follow-up clinic in 1 week
D) Management cheat sheet
First-line
- Adrenaline (1:1000) 0.5 mg IM stat in adult
- Repeat every 5 min if not improved
Supportive
- remove trigger
- lay flat, elevate legs
- oxygen if SpO2 <94%
- IV access
- NSS bolus
- monitor vital signs frequently
If bronchospasm
- Salbutamol nebulization
Adjuncts
- antihistamine
- steroidThese are not first-line.
If poor response after 2 IM doses
- consider IV adrenaline infusion with ECG monitoring
E) Observation / disposition
- observe for biphasic reaction at least 4 hours after improvement
- admit if severe, repeated adrenaline needed, airway involvement, shock, asthma, arrhythmia, beta-blocker use, or poor home observation
F) Ultra-high-yield memory
Anaphylaxis = acute allergy + airway / breathing / circulation problem First drug = IM adrenaline Treat first, labs later Observe for at least 4 hours
1. Introduction
Anaphylaxis is a severe, life-threatening systemic hypersensitivity reaction characterized by rapid onset and potential progression to airway obstruction, respiratory failure, or circulatory collapse. Immediate recognition and treatment are critical, as delayed management significantly increases morbidity and mortality.
2. Definition of Anaphylaxis
Anaphylaxis is diagnosed clinically, not by laboratory tests.
Diagnostic Criteria (Simplified for Exams)
Anaphylaxis is highly likely when there is:
A. Acute onset (minutes–hours) with:
- Skin/mucosal involvement(urticaria, flushing, angioedema)
PLUS at least one of:
- Respiratory compromise(dyspnea, wheeze, stridor, hypoxia)
- Reduced blood pressure or end-organ dysfunction(syncope, hypotension)
B. OR hypotension/airway compromise after allergen exposure
(even without skin findings)
⚠️ Exam Pearl
- ❗ No rash ≠ not anaphylaxis
- ❗ Airway symptoms + hypotension = anaphylaxis until proven otherwise
3. Pathophysiology (High-yield)
- Trigger → IgE-mediated mast cell activation
- Release of mediators:
- Histamine
- Leukotrienes
- Prostaglandins
Effects:
- Vasodilation → hypotension
- Increased permeability → edema (angioedema)
- Bronchoconstriction → wheezing
- Mucosal edema → airway obstruction
4. Clinical Features
Skin
- Urticaria, pruritus
- Angioedema (lips, tongue, eyelids)
Respiratory
- Dyspnea, wheezing
- Stridor, hoarseness (⚠️ airway obstruction)
Cardiovascular
- Hypotension
- Tachycardia, shock
Gastrointestinal
- Abdominal pain, vomiting, diarrhea
🚨 Red Flags (Severe)
- Tongue swelling
- Voice change
- Stridor
- Hypotension
- Altered consciousness
5. Management of Anaphylaxis
Management Setting
➡️ Emergency / IPD (Inpatient)Because risk of:
- Airway obstruction
- Shock
- Biphasic reaction
Primary Survey (ABCDE Approach)
A – Airway
- Look for:
- Tongue swelling
- Hoarseness
- Stridor
- Prepare for early intubation
B – Breathing
- Assess RR, SpO₂
- Give high-flow oxygen
C – Circulation
- Monitor BP, pulse
- Establish IV access
D – Disability
- GCS, mental status
E – Exposure
- Look for rash, urticaria
6. Definitive Treatment (MOST IMPORTANT)
✅ Epinephrine (Adrenaline) — FIRST LINE
Dose:
- Adult: Adrenaline (0.5 mg), 1×1 IM, repeat every 5 min if needed
- Child: 0.01 mg/kg IM
📌 From CMU guideline:
- Max adult dose = 0.5 mg
💡 Why Epinephrine?
- Vasoconstriction → ↑ BP
- Bronchodilation → ↓ wheeze
- ↓ mucosal edema → protects airway
❗ Exam Rule
✅ Give immediately ❌ DO NOT wait for labs ❌ DO NOT start with an antihistamine or a steroid
7. Supportive Management
Fluids
- Normal saline bolus
- Adult: 500–1000 mL IV
- Child: 10 mL/kg
Oxygen
- If SpO₂ < 94% → give oxygen
Monitoring
- Vital signs every:
- 10–15 min if unstable
- 30–60 min if stable
Bronchodilator
- For bronchospasm:
- Salbutamol nebulization
8. Adjunct Medications (NOT FIRST LINE) ❗ Antihistamines
- Chlorpheniramine 10 mg IV q6 hr
- Only improves skin symptoms
❗ Corticosteroids
- Hydrocortisone / methylprednisolone
- Role:
- Reduce prolonged inflammation
- NOT life-saving in the acute phase
❌ Key Exam Trap
- Steroid ≠ emergency treatment
- Antihistamine ≠ airway protection
9. Special Situations
Beta-blocker patient
- May have refractory shock
Treatment:
- Glucagon IV
- Atropine if bradycardia
10. Laboratory Workup
⚠️ Important Rule
👉 Diagnosis is clinical → DO NOT delay treatment
1. Confirm Diagnosis
Serum tryptase
- Take:
- Immediately
- Repeat at 24 hours if admitted
2. Severity Monitoring
- CBC
- Electrolytes
- Renal function
- ABG (if severe)
- ECG (if unstable)
3. Identify Cause (Later)
- Allergy testing
- Specific IgE
- Detailed history
11. Observation & Disposition
Observe for a biphasic reaction
- At least 4 hours after symptom improvement
Admit if:
- Severe anaphylaxis
- 1 dose epinephrine
- Airway involvement
- Comorbid disease (asthma, arrhythmia)
- Lives far / cannot observe symptoms
12. Discharge Plan
Epinephrine auto-injector
- ≥30 kg → 0.3 mg ×2 doses
- <30 kg → 0.15 mg ×2 doses
Follow-up
- Allergy clinic in 1 week
Patient education
- Avoid trigger
- Recognize early symptoms
- Use epinephrine immediately
13. Key Exam Summary
🔑 “EPI FIRST, EVERYTHING ELSE LATER”
| Step | Action |
| 1 | IM Epinephrine |
| 2 | Oxygen + IV fluid |
| 3 | Monitor vital signs |
| 4 | Bronchodilator if wheeze |
| 5 | Antihistamine/steroid (adjunct only) |
14. High-Yield MCQ Pearls
- First-line drug: Epinephrine IM
- Most dangerous sign: Airway edema (stridor, tongue swelling)
- Diagnosis: Clinical, not lab
- Observation: ≥4 hours
- Biphasic reaction: can recurrent later
Conclusion
Anaphylaxis is a time-critical emergency requiring immediate IM epinephrine, aggressive supportive care, and close monitoring. Laboratory tests support diagnosis but must never delay treatment. Early recognition and correct management are essential to prevent mortality.