Hiccups (Singultus): Pathophysiology and Clinical Management
On this page
Introduction
Hiccups (singultus) are involuntary, repetitive contractions of the diaphragm and intercostal muscles, followed by sudden closure of the glottis, producing the characteristic “hic” sound.
While most cases are benign and self-limited, persistent (>48 hours) or intractable (>1 month) hiccups may indicate serious underlying pathology and require systematic evaluation and management.
Pathophysiology of Hiccups
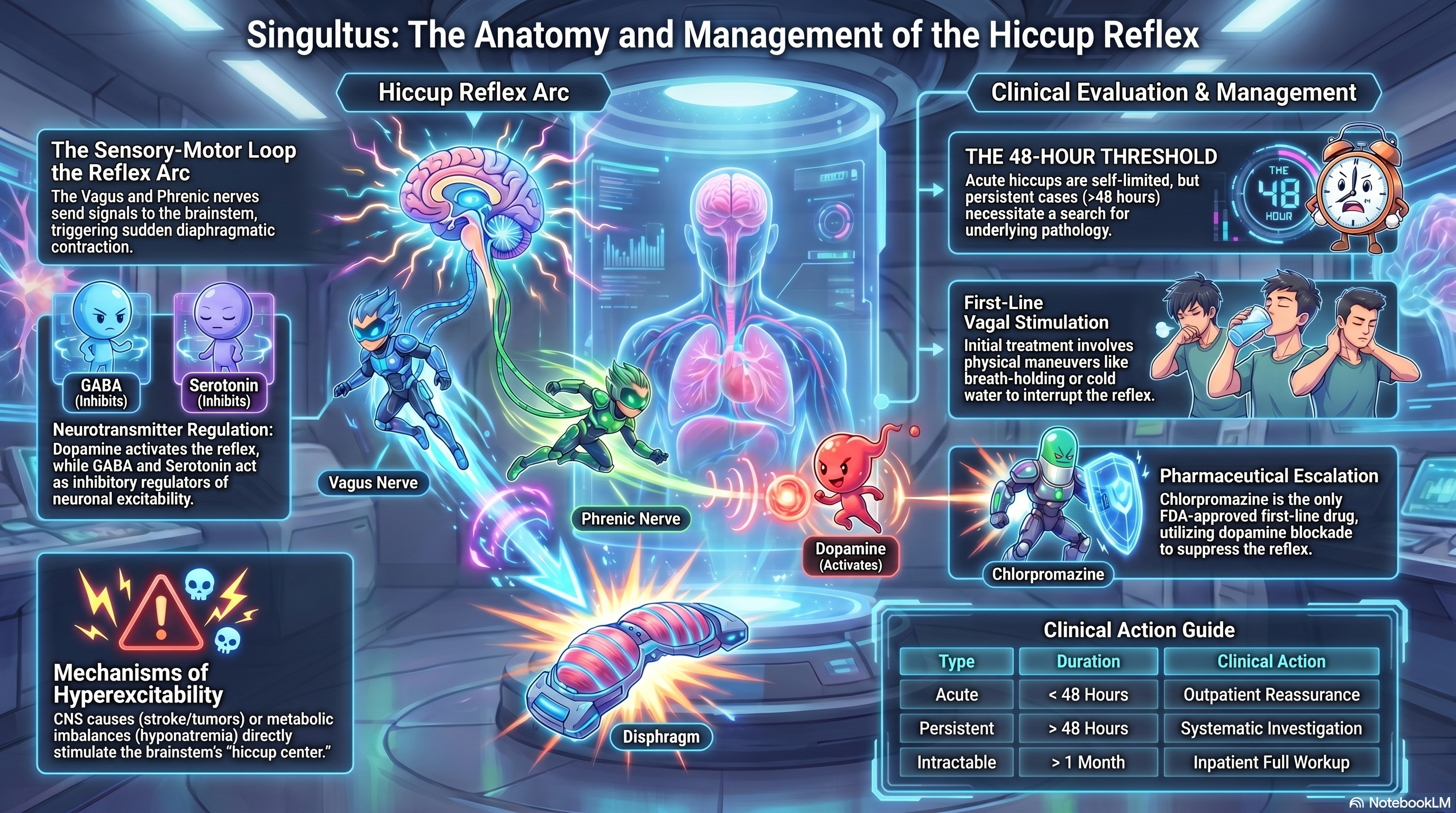
The Hiccup Reflex Arc
Hiccups occur due to dysfunction in a reflex arc, consisting of:
🔹 Afferent limb (sensory input)
- Vagus nerve
- Phrenic nerve
- Sympathetic chain (T6–T12)
👉 Triggered by:
- Gastric distension
- Irritation of the diaphragm
- Thoracic/abdominal pathology
🔹 Central processing unit
- Located in the brainstem (medulla oblongata)
- Sometimes referred to as the “hiccup center.”
👉 Neurotransmitters involved:
- Dopamine (important for reflex activation)
- GABA
- Serotonin
🔹 Efferent limb (motor output)
- Phrenic nerve → diaphragm contraction
- Accessory nerves → intercostal muscles
- Recurrent laryngeal nerve → glottic closure
⚡ Mechanism of Hiccup
- Sudden diaphragmatic contraction
- Rapid inspiration
- Immediate closure of the glottis
- → produces “hic” sound
Pathological Mechanisms
Hiccups arise from hyperexcitability of the reflex arc, caused by:
1. Peripheral irritation
- Gastric distension (overeating, carbonated drinks)
- GERD
- Hepatic or diaphragmatic irritation
2. Central nervous system causes
- Stroke
- Brain tumor
- Meningitis
👉 These directly stimulate the hiccup center
3. Metabolic causes
- Hyponatremia
- Hypocalcemia
- Uremia
👉 Alter neuronal excitability
4. Pharmacologic causes
- Steroids
- Benzodiazepines
- Chemotherapy agents
👉 Affect neurotransmitters (especially dopamine)
🧩 Summary of Pathophysiology
👉 Final common pathway:
Overactive hiccup reflex arc → repetitive diaphragm contraction
🏥 Clinical Management of Hiccups
1. Determine Severity and Setting
| Type | Duration | Management |
| Acute | < 48 hr | OPD, reassurance |
| Persistent | > 48 hr | Investigate |
| Intractable | > 1 month | IPD + full workup |
🚨 Red Flags (MUST NOT MISS)
- Neurological deficits
- Weight loss
- Chest pain
- Persistent vomiting
👉 Requires:
- CXR
- Electrolytes
- CT brain
- Endoscopy
🩺 Management Approach
🔹 1. Treat Underlying Cause (Definitive Treatment)
Examples:
- GERD → Omeprazole (20 mg) 1×1 po AC for 14 days
- Infection → appropriate antibiotics
- Electrolyte imbalance → correction
👉 This is the MOST IMPORTANT step
🔹 2. Symptomatic Treatment
🥇 A. Non-Pharmacological (First-line)
Stimulate vagus nerve → interrupt reflex:
- Breath holding
- Valsalva maneuver
- Drinking cold water
- Pulling tongue
👉 Exam pearl: Always first step
🥈 B. Pharmacological Treatment
⭐ First-line drug (persistent hiccups)
- Chlorpromazine (25–50 mg) 1×3 po PC for 3–7 days
Mechanism:
- Dopamine (D2) blockade in the brainstem
- Suppresses the hiccup reflex center
👉 Only FDA-approved drug
🥈 Second-line options
1. Metoclopramide
- Metoclopramide (10 mg) 1×3 po AC for 5–7 days
- Dopamine antagonist + prokinetic
2. Baclofen
- Baclofen (5–10 mg) 1×3 po for 7 days
- GABA-B agonist → ↓ neuronal excitability
3. Gabapentin (Refractory cases)
- Gabapentin (300 mg) 1×3 po for 7–14 days
👉 Mechanism:
- ↓ excitatory neurotransmitter release
- Stabilizes neuronal activity
⚖️ Drug Selection Summary
| Drug | Mechanism | Role |
| Chlorpromazine | Dopamine blockade | ⭐ First-line |
| Baclofen | GABA agonist | Second-line |
| Gabapentin | Neuromodulator | Refractory |
❌ What NOT to Do (Important)
- ❌ No antibiotics without infection
- ❌ Avoid steroids (can worsen hiccups)
- ❌ Do not ignore persistent hiccups
🧠 Clinical Pearls (HIGH-YIELD)
- Hiccups = brainstem reflex problem
- First-line drug = Chlorpromazine
- Refractory → Gabapentin / Baclofen
- Always look for a cause if >48 hours
🔍 Monitoring & Follow-up
- Reassess symptom resolution in 3–7 days
- If persistent → further investigations
- Monitor for drug side effects:
- Sedation
- Hypotension
- EPS (chlorpromazine)
📖 Guideline-Based Notes
- Chlorpromazine → FDA-approved for hiccups
- GERD-related hiccups → treat per ACG guideline
- Refractory hiccups → supported by neurology & palliative care literature
🧠 Final Summary
👉 Hiccups are caused by:
Overactivation of a brainstem-mediated reflex arc
👉 Management principle:
- Identify and treat the cause
- Suppress reflex (central acting drugs)
- Escalate therapy if persistent