Community-Acquired Pneumonia (CAP): Severity Assessment, Antibiotic Selection, and ICU Management
On this page
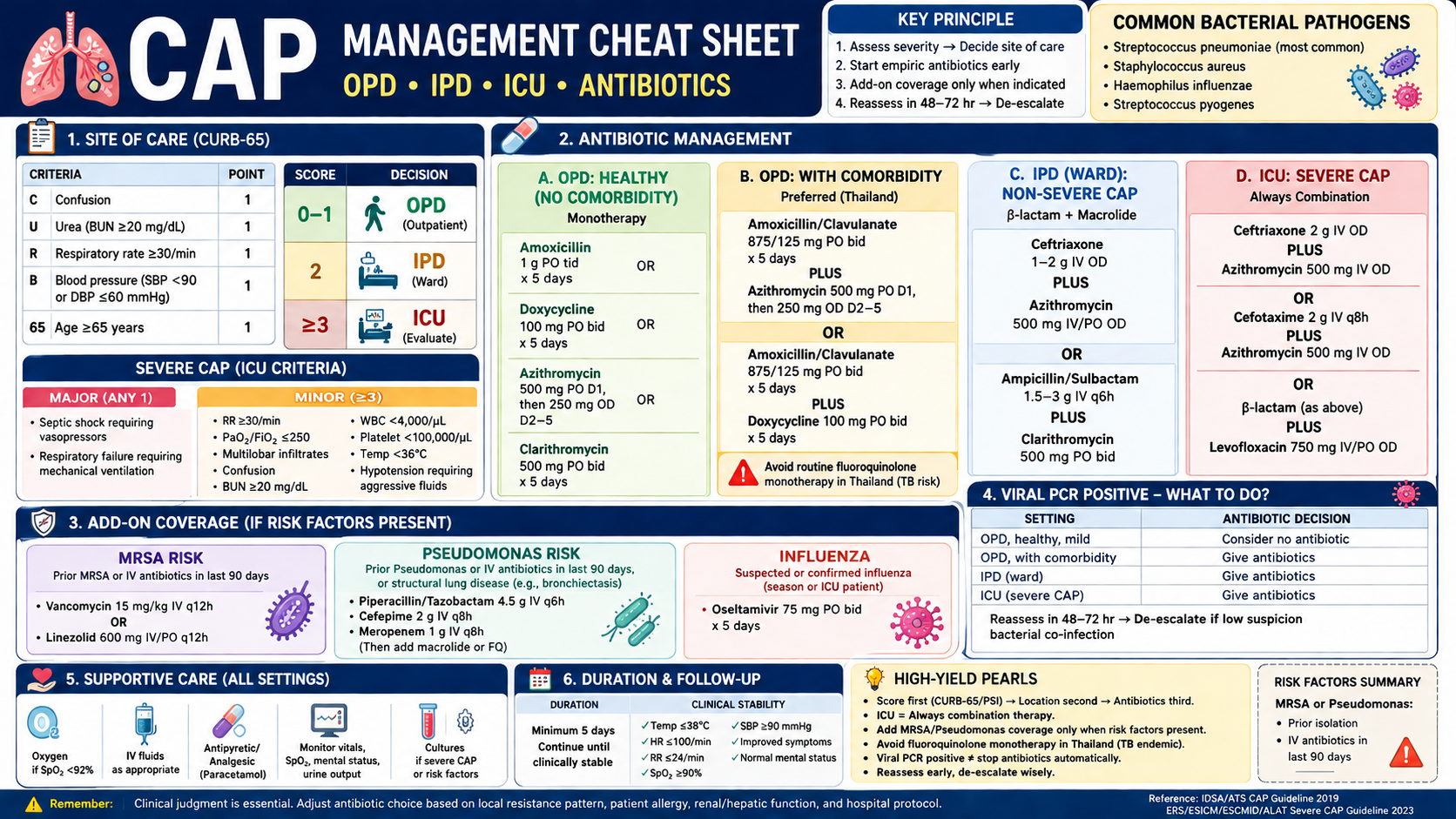
1️⃣ SITE OF CARE
| CURB-65 | Decision |
| 0–1 | ✅ OPD |
| 2 | ✅ IPD |
| ≥3 | 🚨 ICU eval |
2️⃣ OPD MANAGEMENT
| Patient | Antibiotic |
| Healthy | Amoxicillin 1 g tid OR Doxy 100 mg bid |
| Comorbidity | Augmentin + Azithro/Doxy |
| Thailand note | ❌ Avoid FQ mono (TB risk) |
3️⃣ IPD (WARD)
| Severity | Antibiotic |
| Non-severe | Ceftriaxone + Azithromycin |
| Alternative | Amp/Sulbactam + Macrolide |
4️⃣ ICU (SEVERE CAP)
| Rule | Regimen |
| 🔥 Always combo | β-lactam + macrolide |
| Example | Ceftriaxone + Azithro |
5️⃣ ADD-ON COVERAGE
| Condition | Add |
| MRSA risk | Vancomycin / Linezolid |
| Pseudomonas | Pip-Tazo / Cefepime / Meropenem |
| Influenza | Oseltamivir 75 mg bid |
6️⃣ VIRAL PCR POSITIVE
| Setting | Action |
| OPD mild | ± no ABx |
| OPD comorb | ✅ ABx |
| IPD/ICU | ✅ ABx |
| All | Reassess 48–72 hr |
7️⃣ SUPPORT + DURATION
| Item | Plan |
| O₂ | If SpO₂ <92% |
| Duration | ≥5 days |
| Reassess | 48–72 hr |
Community-acquired pneumonia, or CAP, is pneumonia acquired outside the hospital. In real clinical practice, the important question is not only “Does this patient have pneumonia?” but also:
Where should the patient be treated — OPD, IPD ward, or ICU?Which empiric antibiotic should be started?Should we cover MRSA, Pseudomonas, or influenza?
CAP management becomes easy when we follow one rule:
Severity first, antibiotic second.
This article focuses on adult, non-immunocompromised CAP. Immunocompromised patients, active chemotherapy patients, transplant patients, and advanced HIV patients need a separate approach. The IDSA CAP clinical pathway is also designed for adults without immunocompromising conditions.
1. Step One: Decide OPD, IPD, or ICU
Before choosing antibiotics, classify severity.
The main tools are:
| Tool | Best use |
| CURB-65 | Fast bedside tool, practical for exams and wards |
| PSI / Pneumonia Severity Index | More comprehensive, guideline-preferred for site-of-care decision |
| IDSA/ATS severe CAP criteria | Decide whether ICU-level care is needed |
The IDSA pathway uses severity assessment tools such as CURB-65 or PSI to help decide outpatient versus inpatient treatment, then applies severe CAP criteria to identify ICU-level disease.
2. CURB-65: Quick Admission Score
CURB-65 components
Each item = 1 point.
| Letter | Meaning |
| C | Confusion or new disorientation |
| U | Uremia: BUN ≥20 mg/dL |
| R | Respiratory rate ≥30/min |
| B | Blood pressure: SBP <90 mmHg or DBP ≤60 mmHg |
| 65 | Age ≥65 years |
CURB-65 interpretation
| CURB-65 score | Risk | Suggested site of care |
| 0–1 | Low risk | OPD |
| 2 | Moderate risk | IPD ward |
| 3–5 | High risk | IPD + ICU evaluation |
Exam pearl
CURB-65 tells you “Admit or not?”IDSA/ATS severe CAP criteria tell you “ICU or not?”
3. ICU Criteria: Severe CAP
A patient has severe CAP if there is:
1 major criterion OR ≥3 minor criteria
Major criteria
| Major criteria |
| Septic shock requiring vasopressors |
| Respiratory failure requiring mechanical ventilation |
Minor criteria
| Minor criteria |
| RR ≥30/min |
| PaO₂/FiO₂ ≤250 |
| Multilobar infiltrates |
| Confusion/disorientation |
| BUN ≥20 mg/dL |
| WBC <4,000/µL |
| Platelet <100,000/µL |
| Core temperature <36°C |
| Hypotension requiring aggressive fluid resuscitation |
The IDSA CAP clinical pathway defines severe CAP using one major criterion or three or more minor criteria, with the same major and minor criteria above.
4. How to Guess the Possible Pathogen in Real Life
In the real world, we cannot know the pathogen immediately. We estimate it from:
- Host setting
- Age
- Comorbidities
- Immunity
- Structural lung disease
- Local epidemiology
- Pneumococcal resistance
- TB prevalence
- Influenza season
- Hospital antibiogram
- CAP severity
- OPD
- IPD ward
- ICU
- Specific risk factors
- Prior MRSA or Pseudomonas isolation
- Recent hospitalization with IV antibiotics
- Post-influenza pneumonia
- Bronchiectasis or advanced structural lung disease
5. OPD CAP Antibiotic Management
About many CAP cases can be managed as outpatient if severity is low and the patient has no hypoxemia, unstable vital signs, inability to take oral drugs, or serious social risk.
A. OPD CAP: Healthy adult, no comorbidity
This means no chronic heart, lung, liver, or renal disease; no diabetes; no alcoholism; no malignancy; and no asplenia.
Preferred monotherapy options
| Drug | Dose |
| Amoxicillin | Amoxicillin (1000 mg) PO tid for 5 days |
| Doxycycline | Doxycycline (100 mg) PO bid for 5 days |
| Azithromycin | Azithromycin (500 mg) PO day 1, then 250 mg PO OD day 2–5 |
| Clarithromycin | Clarithromycin (500 mg) PO bid for 5 days |
Macrolide monotherapy should only be used when local pneumococcal macrolide resistance is low; this is why many settings prefer amoxicillin or doxycycline first. The ATS/IDSA 2019 CAP guideline is the core reference for these outpatient and inpatient antibiotic strategies. (IDSA)
B. OPD CAP with comorbidities
Comorbidities include:
- Chronic heart disease
- Chronic lung disease
- Chronic liver disease
- Chronic renal disease
- Diabetes mellitus
- Alcoholism
- Malignancy
- Asplenia
Standard guideline option
Use:
Beta-lactam + macrolide/doxycyclineORRespiratory fluoroquinolone monotherapy
Practical Thai approach
In Thailand, we usually prefer:
✅ Dual therapy ❌ Avoid routine respiratory fluoroquinolone monotherapy
Why? Because Thailand has a high TB burden, and fluoroquinolones have activity against Mycobacterium tuberculosis. Empiric fluoroquinolone use for presumed pneumonia can partially treat TB, delay diagnosis, and contribute to fluoroquinolone-resistant TB. WHO-derived data report Thailand’s TB incidence at 146 per 100,000 population in 2024, and systematic review evidence notes concern that fluoroquinolones can delay TB diagnosis in respiratory infections. (World Bank Open Data)
Preferred OPD regimen with comorbidities in Thailand
| Regimen | Dose |
| Amoxicillin/clavulanate + azithromycin | Amoxicillin/clavulanate (875/125 mg) PO bid for 5 days + Azithromycin (500 mg) PO day 1, then 250 mg PO OD day 2–5 |
| Amoxicillin/clavulanate + doxycycline | Amoxicillin/clavulanate (875/125 mg) PO bid for 5 days + Doxycycline (100 mg) PO bid for 5 days |
Alternative beta-lactams:
| Drug | Dose |
| Cefpodoxime | Cefpodoxime (200 mg) PO bid |
| Cefuroxime | Cefuroxime (500 mg) PO bid |
Then add:
- Azithromycin, or
- Clarithromycin, or
- Doxycycline
Exam phrase
In TB-endemic settings such as Thailand, CAP with comorbidities is preferably treated with beta-lactam plus macrolide or doxycycline rather than routine fluoroquinolone monotherapy.
6. IPD CAP Antibiotic Management
Hospitalized CAP is divided into:
- Non-severe CAP → general ward
- Severe CAP → ICU
A. Non-severe CAP: IPD ward
Standard regimen
Beta-lactam + macrolide
This is the most practical and Thai-compatible approach.
| Beta-lactam option | Dose |
| Ampicillin/sulbactam | Ampicillin/sulbactam (1.5–3 g) IV q6h |
| Ceftriaxone | Ceftriaxone (1–2 g) IV OD |
| Cefotaxime | Cefotaxime (1–2 g) IV q8h |
| Ceftaroline | Ceftaroline (600 mg) IV q12h |
Add one macrolide:
| Macrolide | Dose |
| Azithromycin | Azithromycin (500 mg) IV/PO OD |
| Clarithromycin | Clarithromycin (500 mg) PO bid |
Common ward order example
Ceftriaxone (2 g) IV OD + Azithromycin (500 mg) IV/PO OD
What about respiratory fluoroquinolone monotherapy?
ATS/IDSA allows respiratory fluoroquinolone monotherapy for some hospitalized non-severe CAP patients, but in Thailand we avoid routine use because of TB concerns. This is a local stewardship adaptation, not because fluoroquinolones do not work for CAP.
B. Severe CAP: ICU
Severe CAP requires combination therapy.
❌ Do not use monotherapy in severe CAP.✅ Always combine a beta-lactam with atypical coverage.
Preferred severe CAP regimen
| Regimen | Dose |
| Ceftriaxone + azithromycin | Ceftriaxone (2 g) IV OD + Azithromycin (500 mg) IV OD |
Alternative:
| Regimen | Dose |
| Cefotaxime + azithromycin | Cefotaxime (2 g) IV q8h + Azithromycin (500 mg) IV OD |
| Ampicillin/sulbactam + azithromycin | Ampicillin/sulbactam (3 g) IV q6h + Azithromycin (500 mg) IV OD |
ATS/IDSA historically allows either beta-lactam + macrolide or beta-lactam + respiratory fluoroquinolone for severe CAP, but the 2023 ERS/ESICM/ESCMID/ALAT severe CAP guideline specifically suggests adding macrolides, not fluoroquinolones, to beta-lactams as empiric therapy in hospitalized severe CAP. (ERS Publications)
Severe CAP exam pearl
ICU CAP = combination therapy.Macrolide is preferred when possible.
7. When to Add MRSA Coverage
Do not cover MRSA for every CAP patient. Add MRSA coverage only when risk is present.
MRSA risk factors
| MRSA risk factors |
| Prior MRSA colonization or infection, especially respiratory isolation |
| Recent hospitalization with parenteral antibiotics within the last 90 days |
The IDSA CAP pathway lists MRSA severe CAP risk factors including hospitalization with parenteral antibiotics in the last 90 days and prior MRSA colonization or isolation, especially from the respiratory tract.
MRSA drugs
| Drug | Dose |
| Vancomycin | Vancomycin (15 mg/kg) IV q12h, adjust by renal function and drug monitoring |
| Linezolid | Linezolid (600 mg) IV/PO q12h |
Clinical clues for MRSA pneumonia
- Post-influenza pneumonia
- Necrotizing pneumonia
- Cavitary lesion
- Rapid severe pneumonia
- Septic shock
8. When to Cover Pseudomonas
Do not use anti-pseudomonal drugs for everyone.
Pseudomonas risk factors
| Pseudomonas risk factors |
| Prior Pseudomonas respiratory isolation |
| Recent hospitalization with parenteral antibiotics within 90 days |
| Advanced structural lung disease, such as bronchiectasis or advanced COPD |
The IDSA CAP pathway separates non-severe and severe Pseudomonas risk assessment and highlights recent hospitalization with parenteral antibiotics, prior respiratory colonization/infection, and advanced structural lung disease.
Anti-pseudomonal beta-lactam options
Replace the usual beta-lactam with one of the following:
| Drug | Dose |
| Piperacillin/tazobactam | Piperacillin/tazobactam (4.5 g) IV q6h |
| Cefepime | Cefepime (2 g) IV q8h |
| Ceftazidime | Ceftazidime (2 g) IV q8h |
| Imipenem | Imipenem (500 mg) IV q6h |
| Meropenem | Meropenem (1 g) IV q8h |
| Aztreonam | Aztreonam (2 g) IV q8h |
Then add atypical coverage:
- Azithromycin, or
- Respiratory fluoroquinolone if appropriate
Example
Piperacillin/tazobactam (4.5 g) IV q6h + Azithromycin (500 mg) IV OD
9. Influenza Pneumonia and Oseltamivir
If influenza is suspected or confirmed, especially in severe CAP or during influenza season, start antiviral therapy early.
| Drug | Dose |
| Oseltamivir | Oseltamivir (75 mg) PO bid for 5 days |
CDC recommends starting oseltamivir as soon as possible for hospitalized patients with suspected or confirmed influenza. (CDC)
Practical rule
✅ Do not wait for PCR if the patient has severe CAP during influenza season. ✅ Give oseltamivir early, then adjust when PCR returns.
10. CAP with Positive Respiratory Virus PCR: Do We Still Give Antibiotics?
This is a common exam and ward trap.
A positive viral PCR does not always mean “no antibiotics.” Viral infection can predispose to bacterial co-infection, especially in older patients, comorbid patients, and severe CAP.
Practical approach
| Situation | Antibiotic decision |
| Healthy OPD, no comorbidity, strong viral picture, low bacterial suspicion | May withhold antibiotics with close follow-up |
| OPD with comorbidities | Give empiric antibiotics |
| IPD non-severe CAP | Give empiric antibiotics |
| Severe CAP / ICU | Give empiric antibiotics |
| Influenza suspected or confirmed | Add oseltamivir |
The 2025 ATS CAP update suggests not prescribing empiric antibiotics for selected low-risk outpatients without comorbidities who have CAP and a positive respiratory virus test, but it suggests empiric antibiotics for outpatients with comorbidities, non-severe inpatients, and severe CAP because of concern for bacterial-viral coinfection.
Common bacterial co-infection organisms
- Streptococcus pneumoniae
- Staphylococcus aureus
- Haemophilus influenzae
- Streptococcus pyogenes
Exam phrase
Positive viral PCR does not automatically stop CAP antibiotics. In comorbid, IPD, or ICU patients, treat empirically first, then de-escalate.
11. Supportive Management
Antibiotics are not the whole treatment. CAP management also needs respiratory support and general care.
OPD supportive care
- Rest
- Adequate oral hydration
- Antipyretic:
- Paracetamol (500–1000 mg) PO q6h PRN
- Return precautions:
- Worsening dyspnea
- Persistent high fever
- Confusion
- Cyanosis
- Hypotension
- Poor oral intake
- SpO₂ dropping
IPD supportive care
General IPD order style:
- Admit
- Monitor vital signs and oxygen saturation
- Consider I/O monitoring if unstable, elderly, septic, renal disease, or heart failure
- Oxygen therapy if hypoxemic
- IV fluid if dehydrated or septic, but avoid overload
- Blood culture/sputum culture if severe CAP or MRSA/Pseudomonas risk
- Start antibiotics early
- Reassess within 48–72 hours
Clinical stability in hospitalized CAP includes improvement in fever, heart rate, respiratory rate, oxygenation, blood pressure, and mental status; the IDSA pathway lists stability markers such as Tmax ≤38°C, HR ≤100, RR ≤24, oxygen saturation ≥90%, baseline mental status, and SBP ≥90 mmHg.
12. De-escalation and Duration
Reassess at 48–72 hours
Ask:
- Is the patient clinically improving?
- Are cultures positive?
- Is MRSA nasal PCR negative?
- Is viral PCR positive with low bacterial suspicion?
- Is procalcitonin low or falling, if used by the hospital?
The IDSA CAP pathway supports stewardship reassessment and states that antibiotics may be discontinued when viral diagnostics are positive, procalcitonin is low or decreased substantially, WBC is <10,000/µL, and bacterial co-infection suspicion is low.
Duration
For many exam settings, write:
Treat for at least 5 days and until clinical stability.
Modern ATS guidance allows shorter courses in selected clinically stable outpatients and non-severe inpatients, with a minimum of 3 days, but severe CAP should receive ≥5 days.
Practical exam-safe answer
CAP antibiotics: usually 5 days, reassess after 48–72 hours, extend if unstable, severe CAP, MRSA, Pseudomonas, abscess, empyema, or bacteremia.
13. Steroid Note
Steroids are not routine for ordinary non-severe CAP.
The 2025 ATS update recommends not administering systemic corticosteroids in non-severe CAP, while suggesting systemic corticosteroids only for severe CAP, excluding severe influenza pneumonia.
Exam pearl
❌ No routine steroid in non-severe CAP. ❌ Avoid steroid in influenza pneumonia unless another clear indication exists. ✅ Consider steroid only in selected severe CAP according to guideline/local protocol.
14. Full CAP Management Flowchart
Suspected CAP
↓
Confirm pneumonia:
new infiltrate + respiratory symptom + fever/leukocytosis/hypoxia/abnormal lung sound
↓
Assess severity:
PSI or CURB-65
↓
CURB-65 0–1 / PSI I–III
→ OPD treatment
↓
CURB-65 2 / PSI IV–V
→ IPD ward treatment
↓
1 major or ≥3 minor IDSA/ATS severe CAP criteria
→ ICU treatment
↓
Then ask:
MRSA risk?
Pseudomonas risk?
Influenza season/PCR?
Positive viral PCR?
TB possibility?
↓
Choose antibiotic + supportive care
↓
Reassess at 48–72 hours
↓
De-escalate or continue
15. Final High-Yield Summary
| Clinical setting | Preferred treatment |
| OPD, healthy adult | Amoxicillin or doxycycline |
| OPD with comorbidities | Amoxicillin/clavulanate + azithromycin or doxycycline |
| OPD with comorbidities in Thailand | Prefer dual therapy; avoid routine fluoroquinolone monotherapy because of TB concern |
| IPD non-severe CAP | Beta-lactam + macrolide |
| ICU severe CAP | Beta-lactam + macrolide, always combination |
| MRSA risk | Add vancomycin or linezolid |
| Pseudomonas risk | Use anti-pseudomonal beta-lactam + atypical coverage |
| Influenza suspected/confirmed | Add oseltamivir |
| Viral PCR positive + comorbidity/IPD/ICU | Still give empiric antibiotics initially |
| Stable after 48–72 hours | De-escalate based on cultures and clinical response |
Take-home message
CAP treatment is not just “give ceftriaxone.” The correct approach is:
Score severity → decide OPD/IPD/ICU → choose empiric antibiotics → add MRSA/Pseudomonas/influenza coverage only when indicated → reassess and de-escalate.
For Thailand, the most important local adaptation is:
Avoid routine respiratory fluoroquinolone monotherapy when beta-lactam-based dual therapy is appropriate, because TB is common and fluoroquinolones can delay TB diagnosis.