Epstein–Barr Virus (EBV): Pathophysiology, Infectious Mononucleosis, and Management
On this page
Introduction
Epstein–Barr Virus (EBV) is a double-stranded DNA virus from the Herpesviridae family (HHV-4). It is one of the most common human viruses worldwide and is the primary cause of infectious mononucleosis (IM).
💡 High-yield fact (exam):
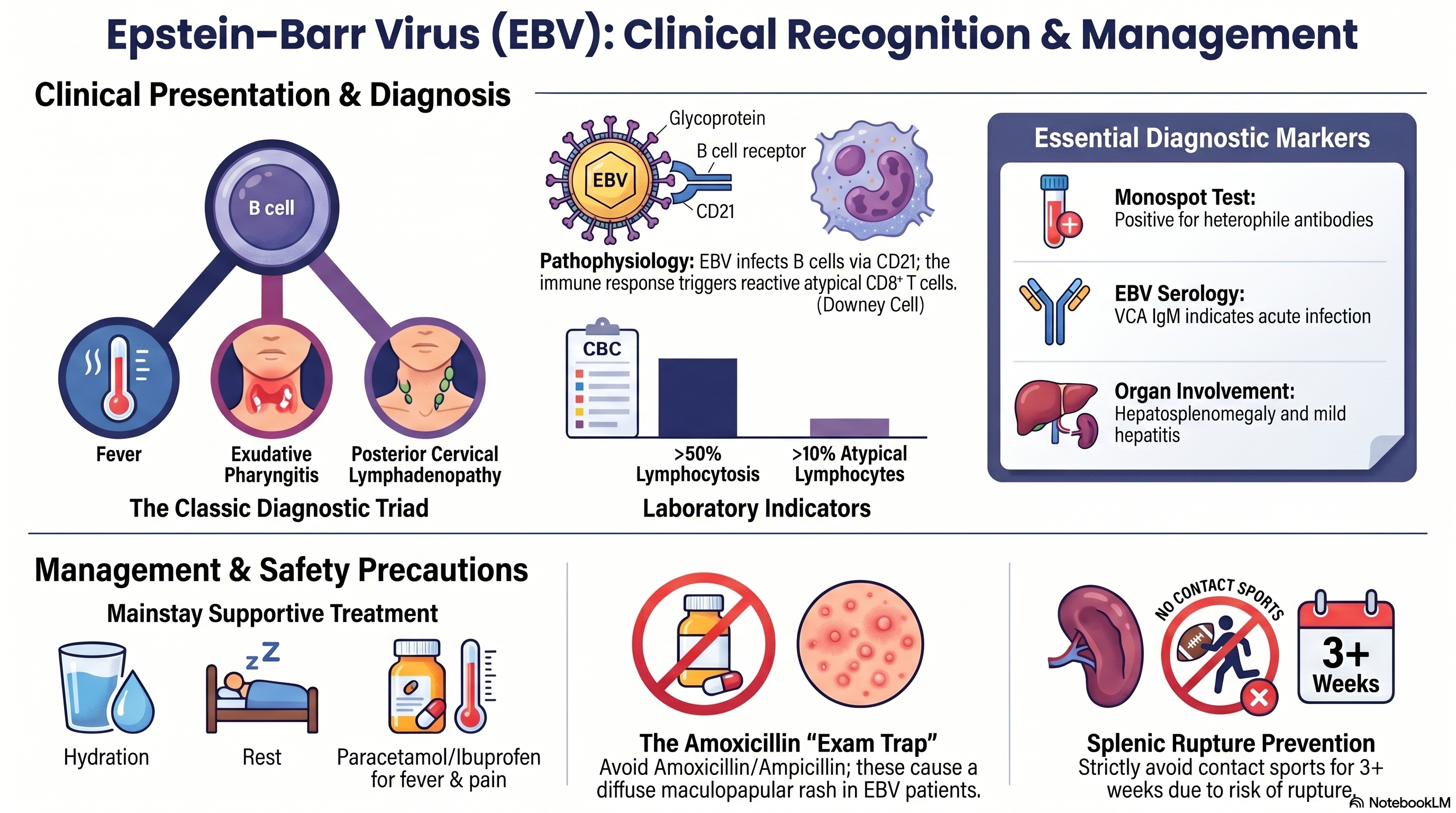
EBV = “Kissing disease” → transmitted via saliva → infects B cells → triggers reactive CD8+ T cells (atypical lymphocytes)
EBV is normally found in which patients?
✅ 1. Age group (MOST IMPORTANT)
- Adolescents & young adults (15–25 years)👉 This group shows classic infectious mononucleosis symptoms
✅ 2. Children
- Often asymptomatic or mild
- Infection occurs early in developing countries
- So they don’t present with classic mono
✅ 3. Transmission risk groups
- Close contact / saliva exposure:
- Kissing (“kissing disease”)
- Sharing drinks, utensils
- Dormitory / school settings
Clinical pattern by age
| Age group | Presentation |
| Children | Asymptomatic / mild |
| Adolescents | Classic mono (fever + sore throat + lymph nodes) |
| Adults | Less typical, sometimes more fatigue |
📌 Immunocompromised patients
- EBV can reactivate → more severe disease
- Associated with:
- Lymphomas
- Post-transplant lymphoproliferative disorder (PTLD)
Exam pearl
If a young adult with severe fatigue + sore throat + posterior cervical lymphadenopathy → think EBV first
One-line summary
EBV is most classically found in adolescents/young adults with infectious mononucleosis, while children are often asymptomatic.
Pathophysiology
Step-by-step mechanism:
- Transmission
- Saliva (kissing, sharing utensils)
- Entry
- Infects oropharyngeal epithelial cells → then B lymphocytes via CD21 receptor
- B-cell infection
- EBV drives B-cell proliferation
- Infected B cells produce heterophile antibodies
- Immune response
- Body activates CD8+ cytotoxic T cells
- These become atypical lymphocytes (Downey cells)
- Organ involvement
- Lymphoid tissue → lymphadenopathy
- Liver → mild hepatitis
- Spleen → splenomegaly (risk of rupture)
- Latency
- Virus persists lifelong in memory B cells
🧠 Clinical Features (Classic Presentation)
🔺 Triad (VERY IMPORTANT for exams)
- Fever
- Pharyngitis (often exudative)
- Lymphadenopathy (posterior cervical)
Other findings
- Severe fatigue (can last weeks)
- Tonsillar enlargement ± exudate
- Palatal petechiae
- Hepatosplenomegaly
- Rash (especially after antibiotics)
🧪 Diagnosis
1. Clinical suspicion
Young adult + sore throat + fatigue + lymph nodes → think EBV
2. Laboratory findings
CBC
- Lymphocytosis (>50%)
- Atypical lymphocytes (>10%)
Heterophile antibody test (Monospot)
- Rapid and commonly used
- May be false negative early (<1 week)
EBV-specific serology
- Used if diagnosis unclear
- VCA IgM → acute infection
🧠 Exam pearl
If “strep throat” is treated but no improvement + fatigue + splenomegaly → think EBV
Lab investigation
Epstein–Barr virus (EBV) infection is typically investigated using a combination of rapid tests and laboratory studies. A commonly used screening test is the heterophile antibody test (Monospot), which provides quick results but may be falsely negative in early disease or in children. Therefore, more specific EBV serology—including VCA IgM (acute infection), VCA IgG (past or current infection), and EBNA IgG (past infection)—is used for confirmation. In addition, a complete blood count (CBC) shows a characteristic pattern: lymphocytosis (>50% lymphocytes) with ≥10% atypical lymphocytes (reactive CD8+ T cells), which is a key diagnostic clue in infectious mononucleosis. Mild thrombocytopenia and slightly elevated liver enzymes may also be present, supporting the diagnosis.
⚠️ Complications (VERY HIGH-YIELD)
1. Splenic rupture 🚨
- Due to splenomegaly
- Risk especially within first 2–3 weeks
- Symptoms:
- LUQ pain
- Referred shoulder pain (Kehr’s sign)
- Hypotension (late)
👉 Prevention:
- ❌ Avoid contact sports ≥ 3 weeks
2. Airway obstruction
- Severe tonsillar enlargement
3. Hematologic
- Hemolytic anemia
- Thrombocytopenia
4. Neurologic (rare)
- Encephalitis
- Guillain-Barré syndrome
5. Malignancy association (long-term)
- Burkitt lymphoma
- Nasopharyngeal carcinoma
- Hodgkin lymphoma
💊 Management (GUIDELINE-BASED)
🏥 Setting: OPD (most cases)
- Self-limiting disease
1. Definitive Treatment
❌ No specific antiviral needed in uncomplicated EBV
- Acyclovir: not routinely recommended
- Steroids: ❌ NOT routine
✅ Use steroids ONLY if:
- Airway obstruction
- Severe hemolytic anemia
- Severe thrombocytopenia
2. Supportive Treatment
- Paracetamol (500 mg) 1×4 po PC → for fever/pain
- Ibuprofen (400 mg) 1×3 po PC (if no contraindication)
- Adequate hydration
- Rest
⚠️ Antibiotic Warning (EXAM TRAP)
❌ Avoid:
- Amoxicillin / Ampicillin
👉 Causes:
- Diffuse maculopapular rash (NOT allergy)
💡 RDU concept:
- Antibiotics are NOT indicated in EBV (viral disease)
BUT ⚠️👉 In your exam, if asked for streptococcal pharyngitis treatment:
- Amoxicillin (500 mg) 1×3 po for 10 daysOR
- Penicillin V (500 mg) 1×3 po for 10 days
🏃 Activity Restriction
- ❌ No contact sports ≥ 3 weeks
- Return when:
- Afebrile
- No splenomegaly (or clinically improved)
🔄 Follow-up
- Re-evaluate in 1–2 weeks
- Monitor:
- Resolution of symptoms
- Signs of complications
🧑⚕️ Patient Education
- Disease is self-limited (2–4 weeks)
- Fatigue may persist longer
- Avoid sharing drinks/kissing during illness
- Return immediately if:
- Severe abdominal pain
- Breathing difficulty
- Persistent high fever
High-Yield Summary
| Topic | Key Point |
| Virus | EBV (HHV-4) |
| Cell infected | B cells (CD21 receptor) |
| Key immune response | CD8+ T cells → atypical lymphocytes |
| Triad | Fever + pharyngitis + posterior cervical nodes |
| Diagnosis | Monospot + atypical lymphocytes |
| Complication | Splenic rupture |
| Avoid | Amoxicillin (rash) |
| Treatment | Supportive only |
Final Clinical Pearl
“Young adult with severe fatigue, exudative pharyngitis, posterior cervical lymphadenopathy, and rash after amoxicillin = EBV infectious mononucleosis until proven otherwise.”