Acute Bacterial Conjunctivitis: Clinical Approach and Treatment Guide
On this page
1. Clinical Definition
Acute bacterial conjunctivitis = superficial infection of the conjunctivaTypical features:
- Red eye
- Mucopurulent discharge (sticky eyelids in morning)
- Mild irritation (NOT severe pain)
- Usually normal vision
2. Determine Severity First (CRITICAL STEP)
Before prescribing anything, classify:
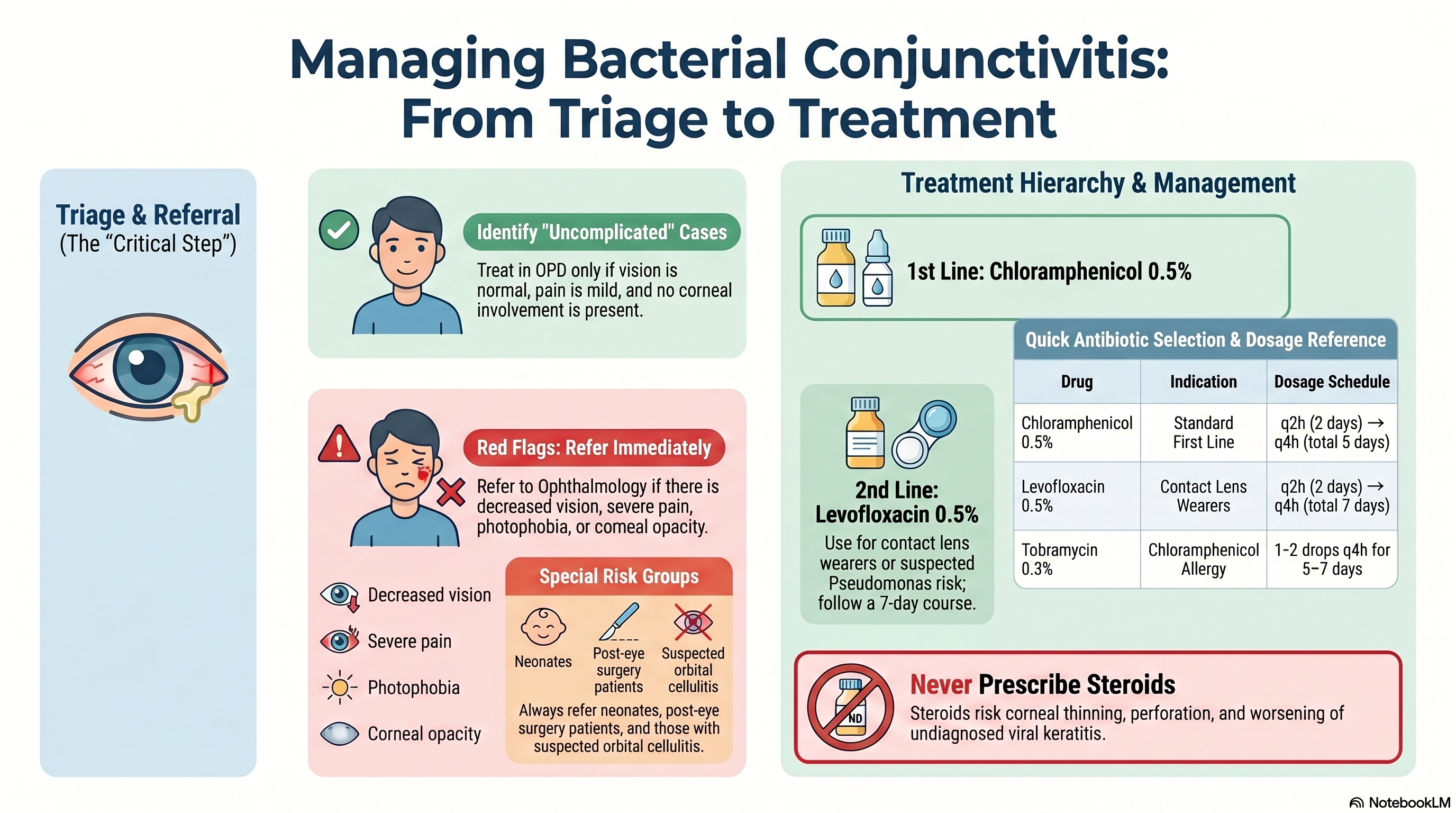
✅ Uncomplicated conjunctivitis (OPD case)
ALL must be present:
- No vision loss
- No severe pain
- No photophobia
- No corneal involvement
- No contact lens–related keratitis suspicion
- No recent eye surgery
- No systemic severe disease
- Not neonate
👉 This is the ONLY group you treat empirically in OPD
❌ Complicated / RED FLAG → REFER OPHTHALMOLOGY
If ANY present:
- ↓ Visual acuity
- Moderate–severe eye pain
- Photophobia
- Corneal opacity / ulcer / keratitis
- Contact lens wearer with red eye
- Pseudomembrane
- Severe unilateral red eye
- Trauma / foreign body
- Post eye surgery
- Neonate
- Suspected orbital/periorbital cellulitis
👉 These are NOT conjunctivitis until proven otherwise
3. Management Setting
👉 Uncomplicated → OPD
No admission needed.
4. Treatment Strategy (Evidence-based + Exam-oriented)
🔑 Key concept (AAO / NICE)
- Many cases are self-limited (5–7 days)
- Antibiotics = shorten duration slightly
- No antibiotic is clearly superior
5. Drug Selection Hierarchy (VERY IMPORTANT)
🥇 FIRST-LINE (Standard answer)
Chloramphenicol 0.5% eye drops
Prescription:
Chloramphenicol (0.5%)1 drop, affected eye(s),q2h while awake × 2 days → then q4h,for 5 days total
Why is this the first line:
✅ Broad coverage (Gram + / Gram –) ✅ Cheap, accessible ✅ Low resistance in community use ✅ Guideline-supported (NICE primary care)
🥈 SECOND-LINE (Special situations)
Levofloxacin 0.5% (Fluoroquinolone)
Prescription:
Levofloxacin (0.5%)1–2 drops, affected eye(s),q2h while awake × 2 days → then q4h,for 7 days
Indications:
✅ Contact lens wearer ✅ Suspected Pseudomonas risk ✅ Concern for early keratitis ✅ Failure of first-line
Why NOT first-line:
❌ Overly broad ❌ Resistance concern ❌ Cost ❌ Stewardship principle
🥉 ALTERNATIVE OPTIONS
1. Tobramycin 0.3%
Prescription:
Tobramycin (0.3%)1–2 drops, affected eye(s),q4h, for 5–7 days
Used when:
- Cannot use chloramphenicol
- Alternative aminoglycoside coverage
2. Poly-Oph (Neomycin + Polymyxin B + Gramicidin)
Prescription:
Poly-Oph1–2 drops, affected eye(s),qid (1×4), for 5–7 days
⚠️ Important Clinical Concerns with Poly-Oph
❌ Why NOT first-line:
- Neomycin → high allergy risk
- Combination = unnecessary for mild disease
- No added benefit vs single-agent therapy
When acceptable:
✅ Mild–moderate infection ✅ Cannot use chloramphenicol ✅ Need broader empirical coverage
When to avoid:
❌ History of drug allergy (especially neomycin) ❌ Suspected viral conjunctivitis ❌ Contact lens-related red eye
6. Supportive Treatment (MUST INCLUDE)
Even if antibiotics given:
- Clean discharge (sterile saline / clean water)
- Hand hygiene
- Avoid touching eyes
- Stop contact lens use
- Warm compress if needed
7. What NOT to do (HIGH-YIELD)
❌ Steroid eye drops→ Risk of:
- Worsening herpes keratitis
- Corneal thinning → perforation
❌ Treat all red eyes as bacterial→ Viral is more common
❌ Use fluoroquinolone routinely→ Resistance + overkill
8. Follow-Up Plan
- Expected improvement: 2–3 days
- Full resolution: ~5–7 days
Re-evaluate if:
- No improvement after 3–5 days
- Symptoms worsen
- New pain / photophobia / vision loss
👉 Then refer to ophthalmology
9. Quick Exam Summary
🧠 Core Answer:
- Uncomplicated → OPD
- 1st line → Chloramphenicol
- Contact lens → Levofloxacin
- Alternative → Tobramycin / Poly-Oph
🔑 Ultimate Clinical Logic
👉 “Most cases are mild → use simple drug” 👉 “Only escalate when risk increases”
🎯 Final Clinical Ordering Template
Diagnosis: Uncomplicated bacterial conjunctivitis
Setting: OPD
Definitive treatment:
- Chloramphenicol (0.5%) 1 drop q2h → q4h × 5 days
Supportive treatment:
- Eye hygiene, warm compress, stop contact lens
Education:
- Avoid contamination
- Return if worse
Follow-up:
- 3–5 days or earlier if red flag