Warfarin/DOAC vs Aspirin: เหตุใดผู้ป่วย Stroke บางรายได้รับยาต่างกัน
- Mayta

- 3 วันที่ผ่านมา
- ยาว 3 นาที
แนวคิดหลัก
ความสับสนเกิดขึ้นเพราะคำว่า "มีประวัติ stroke" ไม่ได้หมายความว่าผู้ป่วยทุกคนต้องได้รับยาป้องกันชนิดเดียวกัน
ผู้ป่วย 2 รายอาจมีประวัติ ischemic stroke เหมือนกัน แต่ สาเหตุของ stroke อาจต่างกัน
✅ ประวัติเหมือนกัน: ischemic stroke ❌ กลไกไม่จำเป็นต้องเหมือนกัน: AF embolus vs atherosclerotic platelet clot ✅ ดังนั้นยาป้องกันจึงไม่จำเป็นต้องเหมือนกัน: anticoagulant vs antiplatelet
หลักสำคัญคือ การป้องกัน stroke ซ้ำต้องดูว่า stroke ครั้งก่อนเกิดจากอะไร
แนวทาง AHA/ASA ด้าน secondary stroke prevention เน้นว่าการป้องกันควรอิงตามสาเหตุของ stroke ครั้งแรก และ guideline AF ปี 2023 (ACC/AHA) ระบุว่าผู้ป่วย AF ที่ต้องการป้องกัน stroke ควรได้รับ anticoagulation โดย aspirin ไม่ได้แนะนำให้ใช้แทน anticoagulation [3]
หมายเหตุ: การแบ่ง "fibrin-rich vs platelet-rich clot" ด้านล่างเป็นการอธิบายแบบง่ายเพื่อการเรียนรู้ การเลือกยาจริงยึดตามกลไกที่พิสูจน์แล้วและหลักฐานจาก trial/guideline ไม่ใช่ลักษณะของ clot เพียงอย่างเดียว
1. AF-related stroke: ใช้ Warfarin หรือ DOAC
ในผู้ป่วย atrial fibrillation (AF) หัวใจห้องบนบีบตัวไม่มีประสิทธิภาพ ทำให้เลือดไหลช้าและคั่ง โดยเฉพาะใน left atrial appendage (LAA)
เมื่อเลือดคั่ง จะเกิด thrombus ได้ง่าย โดย clot ชนิดนี้มักเป็น fibrin-rich thrombus
ถ้า thrombus หลุดออกมา จะเดินทางไปอุดตันหลอดเลือดสมอง ทำให้เกิด cardioembolic ischemic stroke
เหตุผลในการเลือกยา
เพราะ clot จาก AF เกิดจาก blood stasis + coagulation cascade เป็นหลัก จึงควรใช้ยา:
✅ Anticoagulant
ตัวอย่างยา:
Warfarin
Apixaban
Rivaroxaban
Dabigatran
Edoxaban
WARNING - ข้อยกเว้นสำคัญคือ mechanical heart valve: ในกรณีนี้ DOAC เป็นข้อห้าม (RE-ALIGN trial พบว่า dabigatran แย่กว่า warfarin ทั้ง thromboembolism และเลือดออก) ต้องใช้ warfarin เท่านั้น ทุกที่ในบทความที่เขียนว่า "warfarin หรือ DOAC" หมายถึง AF ชนิด non-valvular
ใน non-valvular AF แนวทางปัจจุบันมักแนะนำ DOAC มากกว่า warfarin (2023 ACC/AHA, Class 1) สำหรับผู้ป่วยส่วนใหญ่ ส่วน warfarin ยังเป็นตัวเลือกแรกใน mechanical valve และ moderate-to-severe mitral stenosis
จำง่าย
AF → atrial thrombus → embolic stroke → anticoagulant
2. Non-cardioembolic stroke: มักใช้ Aspirin
ผู้ป่วยบางรายเกิด ischemic stroke จาก atherosclerosis หรือ small-vessel disease ไม่ใช่จาก AF
ตัวอย่างเช่น:
Carotid artery plaque
Intracranial artery stenosis
Lacunar stroke จาก small-vessel disease
Prior TIA หรือ ischemic stroke โดยไม่มี AF
clot กลุ่มนี้มักเป็น platelet-rich clot โดยเฉพาะกรณีที่เกี่ยวข้องกับ plaque rupture หรือ arterial plaque
เหตุผลในการเลือกยา
เพราะ clot เกิดจาก platelet aggregation เป็นหลัก จึงควรใช้ยา:
✅ Antiplatelet
ตัวอย่างยา:
Aspirin 81 mg PO once daily
Clopidogrel
Aspirin/dipyridamole ในบางกรณี
จำง่าย
Atherosclerosis/small-vessel stroke → platelet clot → aspirin หรือ antiplatelet
แนวทาง AHA/ASA ด้าน secondary stroke prevention แนะนำให้ผู้ป่วยเกือบทุกรายหลัง ischemic stroke/TIA ได้รับยาต้านการแข็งตัวของเลือด แต่ชนิดของยาขึ้นกับกลไก: anticoagulation สำหรับ cardioembolism จาก AF และ antiplatelet สำหรับ non-cardioembolic stroke หลายชนิด [2]
ข้อควรระวังเรื่อง ESUS: ในกรณี embolic stroke of undetermined source (ไม่พบ AF หรือแหล่ง cardioembolic ชัดเจน) trials (NAVIGATE-ESUS, RE-SPECT ESUS) พบว่า anticoagulation แบบ empiric ไม่ได้ดีกว่า aspirin ดังนั้นการแบ่ง AF / ไม่ AF จึงไม่ตายตัว antiplatelet ยังเป็นมาตรฐานจนกว่าจะพบแหล่ง cardioembolic
3. ทำไมผู้ป่วยมีประวัติ stroke เหมือนกัน แต่ได้ยาต่างกัน
Patient A
ประวัติ:
Ischemic stroke
มี atrial fibrillation
Stroke น่าจะเกิดจาก cardioembolism
การรักษา:
✅ Warfarin หรือ DOAC
เหตุผล:
AF ทำให้เกิด clot ใน left atrium
Clot หลุดไปสมอง
Anticoagulant ป้องกัน fibrin-rich thrombus ได้ดีกว่า
Patient B
ประวัติ:
Ischemic stroke
ไม่มี atrial fibrillation
มี carotid plaque หรือ small-vessel disease
การรักษา:
✅ Aspirin 81 mg PO once daily หรือ antiplatelet ชนิดอื่น
เหตุผล:
Stroke เกิดจาก platelet/plaque mechanism
Aspirin ลด platelet aggregation
4. ทำไม Aspirin ไม่พอสำหรับ AF
Aspirin ออกฤทธิ์ยับยั้ง platelet
แต่ stroke จาก AF ไม่ได้เกิดจาก platelet เป็นหลัก มันเกิดจาก blood stasis ในหัวใจและ coagulation cascade เป็นหลัก
ดังนั้น aspirin จึงป้องกัน AF-related stroke ได้ไม่ดีพอ
เพราะฉะนั้น:
❌ AF + stroke risk → aspirin alone ไม่เพียงพอ ✅ AF + stroke risk → warfarin หรือ DOAC
guideline AF ปี 2023 (ACC/AHA/ACCP/HRS) ระบุชัดเจนว่า aspirin ไม่ว่าจะใช้เดี่ยวหรือร่วมกับ clopidogrel ไม่ได้แนะนำให้ใช้แทน anticoagulation สำหรับป้องกัน stroke ในผู้ป่วย AF ที่เหมาะกับการได้ anticoagulation [3]
5. ตารางตัดสินใจแบบง่าย
สถานการณ์ของผู้ป่วย | ชนิด clot หลัก | ยาป้องกันที่เหมาะสม |
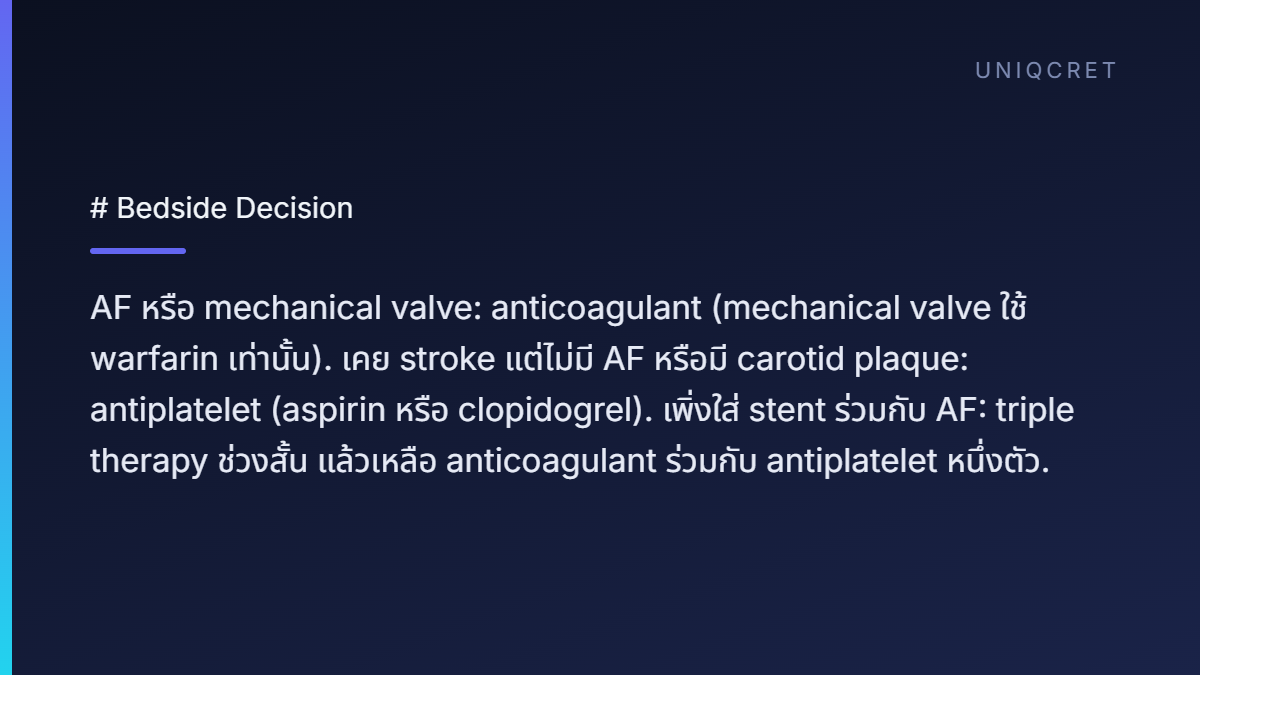
AF with stroke risk | Fibrin-rich atrial thrombus | Warfarin/DOAC |
Mechanical heart valve + stroke risk | Fibrin-rich/prosthetic valve thrombus | Warfarin เท่านั้น (ห้ามใช้ DOAC) |
Prior ischemic stroke without AF | Platelet-rich arterial clot | Aspirin/Clopidogrel |
Carotid artery plaque stroke | Platelet-rich plaque thrombus | Antiplatelet |
Recent coronary stent + AF | มีทั้งสองกลไก | Triple therapy สั้น ๆ แล้วเหลือ OAC + antiplatelet 1 ตัว (P2Y12) |
6. คำอธิบายแบบเข้าใจง่ายสำหรับ HelpCare
ให้คิดว่า stroke prevention คือการเลือก "เครื่องมือให้ตรงกับชนิดของ clot"
Aspirin เป็น antiplatelet drug เหมาะกับ clot ที่เกิดจาก arterial plaque เช่น carotid plaque หรือ coronary plaque เพราะ platelet เป็นตัวสำคัญที่มาเกาะบริเวณ plaque
Warfarin และ DOACs เป็น anticoagulant drugs เหมาะกับ clot ที่เกิดจาก เลือดคั่งในหัวใจ โดยเฉพาะ AF ซึ่งทำให้เกิด fibrin-rich clot ใน left atrium
ดังนั้นคำถามไม่ใช่แค่:
"ผู้ป่วยเคยเป็น stroke หรือไม่?"
แต่ควรถามว่า:
"Stroke ครั้งนั้นเกิดจากสาเหตุอะไร?"
ถ้าสาเหตุคือ AF → ใช้ Warfarin หรือ DOAC ถ้าสาเหตุคือ non-cardioembolic arterial disease → ใช้ Aspirin หรือ antiplatelet
7. One-line memory
✅ AF = Anticoagulant ✅ Atherosclerosis = Aspirin ❌ Aspirin is not a substitute for anticoagulation in AF
เอกสารอ้างอิง
Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2021;52(7):e364-e467.
Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and TIA (full text). Stroke. 2021;52(7):e364-e467.
Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation. Circulation. 2024;149(1):e1-e156.
Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves (RE-ALIGN). N Engl J Med. 2013;369(13):1206-1214.
Hart RG, Sharma M, Mundl H, et al. Rivaroxaban for stroke prevention after embolic stroke of undetermined source (NAVIGATE ESUS). N Engl J Med. 2018;378(23):2191-2201.
Diener HC, Sacco RL, Easton JD, et al. Dabigatran for prevention of stroke after embolic stroke of undetermined source (RE-SPECT ESUS). N Engl J Med. 2019;380(20):1906-1917.



ความคิดเห็น