Median Raphe Cyst: Types, Diagnosis & Treatment of Midline Genital Lesions in Males
On this page
Introduction
Median raphe cysts are benign, congenital lesions that form anywhere along the midline raphe of the male genitalia — from the meatus of the penis, along the scrotum, down to the perineum. They develop from trapped epithelial tissue during embryogenesis and are often unrecognized until adolescence or adulthood.
🔬 Pathophysiology
During embryonic development, incomplete closure or epithelial fusion along the urethral and scrotal midline can result in epithelial-lined cysts. These remain silent and slowly grow, sometimes forming visible or palpable nodules.
👀 Clinical Morphological Types
Median Raphe Cyst
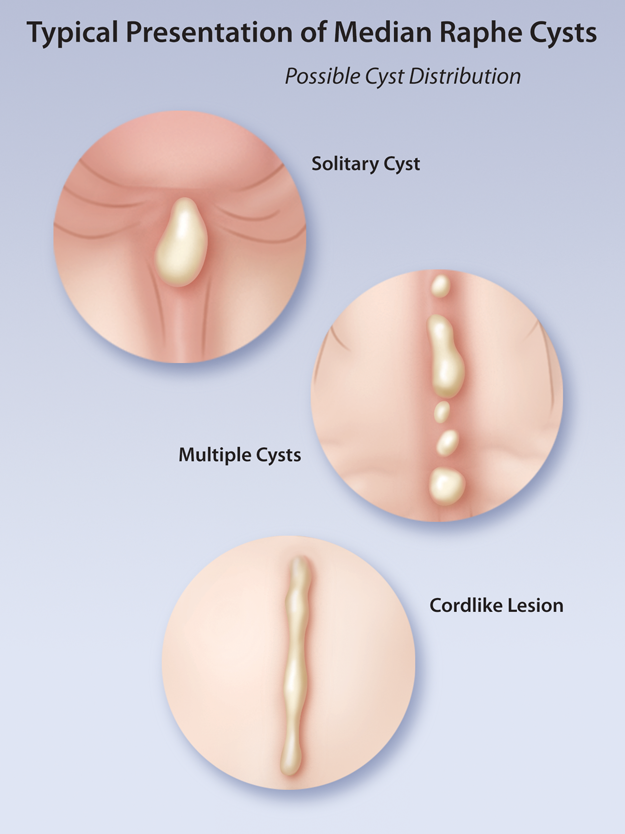
Image source:
HealthPlexus: Median Raphe Cysts
Copyright belongs to the original publisher.
Based on the illustration provided, median raphe cysts can appear in different forms:
1. 🔹 Solitary Cyst
- Presentation: A single, small, dome-shaped, yellowish or skin-colored nodule.
- Common site: Scrotal or penile midline.
- Typical concern: Cosmetic appearance or occasional discomfort.
- Key Feature: Non-tender, non-inflammatory, may be compressible.
2. 🔸 Multiple Cysts
- Presentation: Several cystic nodules distributed in a segmental line along the raphe.
- Clinical significance: Rare but notable for possible irritation from clothing or friction.
- Key Feature: Separate small nodules that may appear simultaneously or sequentially.
3. 🔹 Cordlike Lesion
- Presentation: A linear or sausage-like swelling along the raphe, composed of coalescing small cysts.
- Commonly mistaken for: Epidermal inclusion cyst chain or penile lymphangiectasia.
- Key Feature: Rope-like, soft to firm texture, non-tender unless secondarily infected.
⚠️ Important Clinical Points
✅ Positive Findings:
- Midline location (unique feature).
- Soft, cystic, mobile, non-painful lesion.
- No erythema or warmth unless infected.
❌ Negative Findings:
- No redness or swelling unless infected.
- No fever, systemic signs.
- No lymphadenopathy.
🔍 Differential Diagnosis
| Condition | Differences from MRC |
| Epidermoid cyst | Often lateral; filled with keratin. |
| Furuncle | Painful, red, pus-filled. |
| Hydrocele | Fluctuant, transilluminates, not midline. |
| Sebaceous cyst | May be midline but more common elsewhere. |
| Scrotal abscess | Fluctuant, painful, febrile. |
🧪 When to Investigate
- Ultrasound (USG): To confirm fluid-filled nature and rule out vascular lesion.
- Swab culture (if discharge present): To rule out infection.
- Biopsy (rare): If diagnosis unclear or rapid growth.
🛠️ Management
| Status | Approach |
| Asymptomatic | Observation and reassurance. No intervention needed. |
| Symptomatic | Surgical excision (curative). Local anesthesia is usually sufficient. |
| Infected | Warm compresses ± antibiotics. Avoid I&D unless necessary. Surgical excision later. |
📋 Patient Advice
Do not scratch or squeeze it like a pimple! Squeezing may cause the secondary infection. The best management if it grows or becomes bothersome is surgical excision.
✅ Take-home Messages
- Median raphe cysts are benign, congenital, and usually painless.
- Three main types: solitary, multiple, and cordlike.
- Surgery is not always needed — only if infected, enlarging, or cosmetically bothersome.
- Avoid manipulation to prevent inflammation or secondary infection.
Comments
No comments yet. Be the first to share your thoughts.
Sign in to comment